Blog > Treatment Strategies > Best Evidence-Based Supplements for Mental Health (2025-2026)
Best Evidence-Based Supplements for Depression & Anxiety: A Clinician's Guide
Looking for the best evidence-based supplements for mental health? Research suggests that certain vitamins, minerals, and nutraceuticals may help support mood, reduce anxiety symptoms, and improve outcomes for some individuals with depression when used alongside evidence-based treatment. This guide reviews the best supplements for depression and anxiety, including omega-3 fatty acids, magnesium, vitamin D, L-methylfolate, NAC, saffron, SAMe, and other mental health supplements. You'll find clinical evidence, recommended dosages, safety considerations, and drug-supplement interaction guidance to help make informed treatment decisions.

Last Updated: May 29, 2026
")
")
What You'll Learn
- The best evidence-based supplements for depression, anxiety, and mental health support
- Typical dosages, evidence ratings, and clinical applications for leading mental health supplements
- How omega-3s, magnesium, vitamin D, L-methylfolate, NAC, saffron, and other nutraceuticals compare
- Common drug-supplement interactions and safety considerations for behavioral health clinicians
- How to match supplement recommendations to common clinical presentations using a practical decision-making framework
- Evidence-backed lifestyle interventions that can improve mood and anxiety outcomes
- How to evaluate supplement quality, monitor outcomes, and integrate nutraceuticals into evidence-based treatment plans
Contents
- Quick Reference: Best Evidence-Based Supplements for Mental Health
- Adjunctive Nutraceuticals that Support Mood and Anxiety
- Herbal and Natural Supplements for Depression and Stress
- Which Mental Health Supplements Have the Strongest Evidence?
- Other Evidence-Informed Options Worth Knowing
- How to Choose the Right Supplement for Depression and Anxiety
- Integrative Approaches: Lifestyle Interventions That Amplify Supplement Effects
- Drug-Supplement Interactions: What Behavioral Health Clinicians Need to Know
- Practical Tips for Integrating Supplements Into Treatment
- FAQ: Best Supplements for Mental Health
- Final Thoughts on Mental Health Supplements
- How ICANotes Supports Clinicians Using Integrative Mental Health Approaches
When patients ask, "What else can I do?" or "Are there natural options?" we now have more research-backed answers than ever before. Over the past decade, high-quality clinical trials and systematic reviews have shown that certain vitamins, supplements, and lifestyle interventions can make a meaningful difference in mood, anxiety, and stress resilience — especially when used alongside traditional treatment.
This guide was written for behavioral health clinicians, including therapists, psychiatrists, psychiatric nurse practitioners, and other professionals supporting individuals with mood and anxiety disorders. It also serves as a valuable resource for patients who want to discuss evidence-based supplement options with their healthcare providers.
A Note on These Recommendations
These strategies are adjuncts, not replacements. For moderate-to-severe depression or anxiety, therapy and/or medication remain first-line. Always screen for contraindications and drug interactions before recommending supplements. See the Drug-Supplement Interaction Reference Card (free download below) for a clinical safety summary.
Quick Reference: Best Evidence-Based Supplements for Mental Health
Use this table for rapid clinical reference. Full dosing guidance, mechanisms, and evidence summaries appear in the sections below.
| Supplement | Best For | Dose | Key Evidence | Evidence Grade | Notes |
|---|---|---|---|---|---|
| Omega-3 (EPA) | Depression, partial SSRI response | 1,000+ mg EPA/day | 26-RCT meta-analysis | A — Strong | EPA > DHA for mood support |
| Vitamin D | Depression, low sun exposure | 2,000–5,000 IU/day | 948-patient meta-analysis | B — Moderate | Check 25(OH)D levels first |
| L-Methylfolate | SSRI augmentation, MTHFR variants | 15 mg/day | Multiple RCTs + meta-analysis | A — Strong | Preferred over folic acid |
| Magnesium | Anxiety, sleep, stress | 248–500 mg/day | 7-RCT meta-analysis | B — Moderate | Glycinate form preferred |
| NAC | Treatment-resistant depression | 2,000–3,000 mg/day | 12-RCT meta-analysis | B — Moderate | Divide into two doses |
| SAMe | Depression augmentation | 200–800 mg/day | Multiple RCTs | A — Strong | Screen for bipolar disorder |
| Saffron | Mild-moderate depression, anxiety | 30 mg/day | 23-RCT review | B — Moderate | Comparable to SSRIs in some studies |
| Ashwagandha | Stress, anxiety, burnout | 500–600 mg/day | 7-RCT meta-analysis | B — Moderate | Use caution with liver disease |
| Zinc | Depression adjunct, deficiency | 15–25 mg/day | Multiple small RCTs | C — Emerging | Most useful when deficient |
| Probiotics | Mood, anxiety, gut-brain axis | Strain dependent | WFSBP statement | C — Emerging | Look for Lactobacillus and Bifidobacterium strains |
Note: Supplements should be used as adjuncts to evidence-based treatment, not as replacements for psychotherapy or medication when clinically indicated.
Best Supplements for Depression and Anxiety at a Glance

This supplement comparison chart summarizes some of the most evidence-based supplements for mental health, including options commonly used to support depression, anxiety, stress resilience, and treatment-resistant mood symptoms. Clinicians should evaluate individual patient needs, medication interactions, and nutritional deficiencies before recommending supplements.
Adjunctive Nutraceuticals that Support Mood and Anxiety
The following supplements have the strongest evidence base for adjunctive use in behavioral health. Each entry includes mechanism, clinical evidence, recommended dosing, and best-fit patient profiles.
Omega-3 for Depression and Anxiety: EPA vs. DHA Explained
Omega-3 fatty acids are among the most studied supplements in psychiatry, but not all omega-3s are equal for mental health. It is the EPA fraction — not DHA — that consistently shows antidepressant effects. A comprehensive 2019 meta-analysis of 26 randomized controlled trials confirmed that EPA-dominant formulations produce significant reductions in depressive symptoms, with the strongest benefits seen in individuals with partial SSRI response or elevated systemic inflammation.
The mechanism is primarily anti-inflammatory: EPA suppresses pro-inflammatory cytokines that are increasingly implicated in treatment-resistant depression. DHA remains important for neurological development and general brain health, but in adults with mood disorders, it is EPA that does the heavy lifting.
Clinical Guidance
Vitamin D Deficiency and Depression: What the Evidence Says
Vitamin D is not just a bone-health nutrient — it plays a direct role in serotonin synthesis and neuroinflammatory regulation. Deficiency is strikingly common in patients with depression, particularly during winter months or in individuals with limited sun exposure, darker skin tones, or indoor lifestyles.
A 2019 meta-analysis of 948 individuals with clinical depression found that vitamin D supplementation produced moderate antidepressant effects even when administered independently of antidepressants. In one notable trial, combining vitamin D with fluoxetine produced significantly greater mood improvement than the SSRI alone.
Clinical Guidance
B Vitamins for Depression: L-Methylfolate and B12 Explained
The B-vitamin complex — particularly L-methylfolate and vitamin B12 — is essential for neurotransmitter synthesis and the methylation cycle. Deficiencies in either can cause fatigue, poor concentration, and low mood that mimics or worsens depression.
L-methylfolate, the bioactive form of folate, has been studied specifically as an SSRI augmentation strategy. In two large clinical trials, 15 mg/day led to significantly greater response rates than placebo in patients with inadequate antidepressant response. A 2022 meta-analysis confirmed these findings, with particularly strong effects in patients with MTHFR polymorphisms or elevated inflammatory markers — a population often missed with standard folic acid supplementation.
Vitamin B12 deficiency is especially common in vegetarians, older adults, and patients on metformin or proton pump inhibitors. Even low-normal B12 levels can blunt antidepressant response.
Clinical Guidance
Magnesium for Anxiety and Depression: Best Forms and Doses
Magnesium is involved in more than 300 enzymatic reactions, many of which directly regulate the nervous system. It acts as a natural NMDA receptor antagonist, supports GABA activity, and helps regulate the HPA (stress response) axis — making it one of the most physiologically relevant supplements for both anxiety and depression.
A 2023 meta-analysis of seven RCTs found a moderate-to-large reduction in depressive symptoms with magnesium supplementation. The form matters: magnesium glycinate offers superior absorption and tolerability compared to magnesium oxide, which is poorly absorbed and more likely to cause gastrointestinal side effects. Magnesium threonate has additional evidence for cognitive support.
Clinical Guidance
N-Acetylcysteine (NAC) for Treatment-Resistant Depression
N-acetylcysteine (NAC) is a glutathione precursor with a dual mechanism relevant to psychiatry: it modulates glutamate transmission and reduces oxidative stress and neuroinflammation. This makes it particularly relevant for patients whose depression has an inflammatory or glutamatergic component.
A 2024 meta-analysis of 12 RCTs found small but statistically significant benefits for depressive symptoms, with the strongest effects in patients with bipolar depression or treatment-resistant unipolar depression. NAC is also being explored for OCD, trichotillomania, and substance use disorders.
Clinical Guidance
Herbal and Natural Supplements for Depression and Stress
SAMe for Depression: One of the Strongest Evidence Bases in Nutraceuticals
S-adenosylmethionine (SAMe) is a naturally occurring methyl donor that participates in the synthesis of serotonin, dopamine, and norepinephrine. Among all nutraceuticals, SAMe has one of the strongest evidence records for depression: multiple double-blind, placebo-controlled RCTs have demonstrated efficacy both as monotherapy and as SSRI augmentation, and it has been incorporated into international treatment guidelines as a second-line adjunct.
Clinical Guidance
Ashwagandha for Stress and Anxiety: Evidence-Based Dosing
Ashwagandha (Withania somnifera) is an adaptogen with among the best clinical evidence of any herbal supplement in the anxiety and stress category. Its primary mechanisms include HPA axis regulation and mild GABA-mimetic effects, which together reduce cortisol levels and improve sleep quality.
A 2021 meta-analysis of seven placebo-controlled trials showed significant reduction in anxiety symptoms with 500–600 mg/day of a standardized extract. Effects were most pronounced in patients with chronic stress, burnout, or anxiety-related insomnia.
Clinical Guidance
Saffron Supplement for Depression: How it Compares to SSRIs
Saffron (Crocus sativus) has quietly become one of the best-studied botanical antidepressants. At just 30 mg/day, it has been shown in multiple RCTs to significantly reduce symptoms of depression and anxiety. A landmark 2019 review of 23 RCTs concluded that saffron’s efficacy was comparable to SSRIs in mild-to-moderate depression — with a far more favorable side effect profile.
The mechanism likely involves mild serotonin reuptake inhibition and antioxidant activity. Because it is extremely well tolerated and gentle, saffron is particularly suited for patients who are sensitive to standard medications, prefer a plant-based approach, or have mild presentations that don’t clearly warrant pharmacotherapy.
Clinical Guidance
Which Mental Health Supplements have the Strongest Evidence?
Not all supplements are supported by the same level of research. Some have been evaluated in multiple randomized controlled trials and meta-analyses, while others show promise but require further study. The evidence strength pyramid below provides a quick visual overview of how commonly recommended mental health supplements compare based on the quality and consistency of the available clinical evidence.

Important: A lower evidence ranking does not mean a supplement is ineffective. It simply reflects the current state of the research. Clinical decision-making should always consider patient presentation, nutritional deficiencies, medication use, treatment history, and individual preferences.
Other Evidence-Informed Options Worth Knowing
Beyond the core supplements and lifestyle practices already discussed, several additional natural compounds are gaining attention for their potential mental health benefits. While these options may not yet be considered first-line adjuncts, emerging research supports their thoughtful use in specific clinical contexts. The following treatments offer promising, though sometimes preliminary, evidence and may be valuable additions to a personalized, integrative mental health plan.
Zinc for Brain Health and Depression
Zinc is a trace mineral essential for BDNF production, neuroplasticity, and neurotransmitter regulation. Low serum zinc levels are consistently associated with depressive symptoms across population studies. Small RCTs have explored zinc as an antidepressant adjunct at 25–30 mg/day of elemental zinc, with mixed but promising results — particularly in patients with documented deficiency.
Zinc deficiency is more common than often recognized, especially in individuals with poor dietary intake, chronic stress, or systemic inflammation. For patients with partial treatment response and suspected nutritional gaps, zinc is a low-cost, low-risk addition. Use zinc picolinate or zinc glycinate for superior bioavailability.
Probiotics for Mood and Anxiety: The Gut-Brain Axis
Gut microbiome research has established a bidirectional link between intestinal health and mental health — the gut-brain axis. Specific strains of Lactobacillus and Bifidobacterium have demonstrated the ability to modulate neurotransmission, reduce systemic inflammation, and improve gut barrier integrity. In 2022, the World Federation of Societies of Biological Psychiatry formally acknowledged probiotics as having “emerging support” for adjunctive use in depression.
Probiotics are best used in patients with mood symptoms alongside gastrointestinal complaints, IBS, or a history of chronic stress that has affected gut health. Strain selection matters; clinical evidence is strongest for multi-strain Lactobacillus/Bifidobacterium products.
Chamomile and Lavender (Silexan) for Anxiety Relief
Chamomile (Matricaria chamomilla) has demonstrated anxiolytic effects in patients with generalized anxiety disorder, with one RCT showing significant symptom reduction over eight weeks. It is gentle, safe, and appropriate for mild anxiety presentations.
Lavender oil in its standardized oral form — Silexan (80 mg/day) — has shown particularly impressive evidence, with multiple trials demonstrating results comparable to low-dose benzodiazepines without the cognitive dulling, sedation, or dependence risk. For patients with mild-to-moderate anxiety, sleep disturbances, or somatic anxiety symptoms, Silexan is a compelling option worth discussing.
How to Choose the Right Supplement for Depression and Anxiety
Not every supplement is appropriate for every patient. The best choice depends on symptoms, treatment history, nutritional status, medication use, and individual preferences. Use the quick-reference decision tree below to match common clinical presentations with evidence-informed supplement options.
Supplement Decision Tree for Mood and Anxiety Support
Use this quick clinical guide to match common patient presentations with evidence-informed adjunctive options.
Depression Symptoms?
Consider:
- Omega-3 EPA
- L-Methylfolate
- SAMe
Anxiety or Stress?
Consider:
- Magnesium Glycinate
- Ashwagandha
- Saffron
Treatment-Resistant Mood Symptoms?
Consider:
- NAC
- SAMe
- L-Methylfolate
Seasonal Symptoms or Low Sun Exposure?
Consider:
- Vitamin D
- Bright Light Therapy
- Exercise
Clinical reminder: These options should be used as adjuncts to evidence-based care, not as replacements for psychotherapy, medication, or medical evaluation when clinically indicated. Always screen for contraindications and drug-supplement interactions.
While supplements can be valuable adjuncts, they are often most effective when combined with lifestyle interventions that target many of the same biological pathways. Exercise, bright light therapy, mindfulness-based cognitive therapy (MBCT), sleep optimization, and nutrition counseling can amplify the benefits of evidence-based supplements and improve long-term outcomes.
Supplements can be valuable adjunctive tools, but they work best as part of a broader treatment strategy. Clinicians looking for additional evidence-based interventions for depression may consider combining nutraceuticals with psychotherapy, exercise, behavioral activation, sleep interventions, and other established approaches.
Integrative Approaches: Lifestyle Interventions That Amplify Supplement Effects
Nutraceuticals work best when paired with lifestyle interventions that target the same biological pathways — inflammation, neuroplasticity, and stress regulation. The following are among the most evidence-supported, and many clinicians find that framing them alongside supplements makes both more acceptable to patients.
Many of the nutrients discussed in this guide can also be obtained through dietary changes, and clinicians may benefit from reviewing these foods that boost mental health when discussing nutrition-based interventions with patients
Bright Light Therapy for Seasonal and Non-Seasonal Depression
Light therapy regulates circadian rhythms and enhances serotonin synthesis. A 2024 meta-analysis confirmed effectiveness in both seasonal and non-seasonal depression. The standard protocol is 10,000 lux for 30 minutes each morning. It is considered a first-line treatment for seasonal affective disorder and a valuable adjunct for patients experiencing circadian disruption. In patients with bipolar disorder, monitor carefully for signs of hypomanic switching.
Exercise as an Antidepressant
A landmark 2023 umbrella review of 218 trials involving more than 14,000 participants found that exercise was as effective as antidepressants for mild-to-moderate depression. Benefits appear to result from increased BDNF, reduced inflammation, improved HPA-axis regulation, and enhanced neuroplasticity. Walking, yoga, and resistance training all demonstrated positive effects. Exercise is only one component of a comprehensive treatment plan, and clinicians may also consider other evidence-based interventions for anxiety when supporting patients with persistent anxiety symptoms.The target is approximately 150 minutes of moderate-intensity activity per week, but for sedentary or depressed patients, starting with any movement is often the most important step.
Mindfulness-Based Cognitive Therapy (MBCT)
MBCT has level-1 evidence for preventing relapse in recurrent depression and is increasingly recommended as a standard-of-care adjunct. It helps reduce rumination, improve emotional regulation, and has been shown in multiple randomized controlled trials to reduce relapse rates by 40–50% in patients with three or more depressive episodes. For individuals prone to anxious thinking or depressive relapse, MBCT apps and group programs offer accessible, low-cost interventions that pair well with nutraceutical strategies.
Drug-Supplement Interactions: What Behavioral Health Clinicians Need to Know
Natural does not mean risk-free. Several commonly recommended supplements carry meaningful interactions with psychiatric medications. Review these before making recommendations, and always document supplement use in the clinical record.
| Supplement | Medication(s) | Interaction Type | Clinical Risk | Recommendation |
|---|---|---|---|---|
| St. John's Wort | SSRIs, SNRIs, MAOIs | Serotonin syndrome; CYP3A4 induction | HIGH — Contraindicated | Do not combine; counsel patients explicitly. |
| St. John's Wort | Oral contraceptives, antiretrovirals, warfarin | Reduces drug efficacy via CYP induction | HIGH | Avoid; broad drug interaction profile. |
| SAMe | SSRIs; undiagnosed bipolar disorder | Serotonin augmentation; hypomanic switch | MODERATE-HIGH | Screen for bipolar spectrum disorders; start low. |
| 5-HTP | SSRIs, MAOIs, tramadol | Serotonin syndrome risk | HIGH — Avoid Concurrent Use | Do not combine without specialist guidance. |
| High-Dose Omega-3 (>3g/day) | Warfarin, aspirin, clopidogrel | Additive antiplatelet/anticoagulant effect | MODERATE | Monitor INR and coagulation status. |
| Ashwagandha | Thyroid medications (levothyroxine) | May increase thyroid hormone levels | MODERATE | Monitor TSH and thyroid function. |
| Ashwagandha | Benzodiazepines, sedatives | Additive CNS depression | LOW-MODERATE | Use cautiously; counsel regarding sedation. |
| Magnesium | Lithium | May affect renal lithium clearance | MODERATE | Monitor lithium levels and hydration status. |
| Magnesium | Quinolone & tetracycline antibiotics | Reduced antibiotic absorption | LOW-MODERATE | Separate administration by at least 2 hours. |
| L-Methylfolate | Valproate, carbamazepine | Drug depletes folate; folate may affect drug levels | MODERATE | Supplementation generally recommended; monitor levels. |
| NAC | Nitroglycerin | Additive vasodilation; hypotension risk | MODERATE | Use cautiously in patients receiving nitrates. |
| Zinc | Copper (long-term high-dose use) | Nutritional imbalance | LOW | Consider 1–2 mg copper supplementation with prolonged zinc use. |
Clinical Note: This table highlights common and clinically significant supplement-drug interactions relevant to behavioral health practice. It is not exhaustive and should not replace consultation of a current drug interaction database.
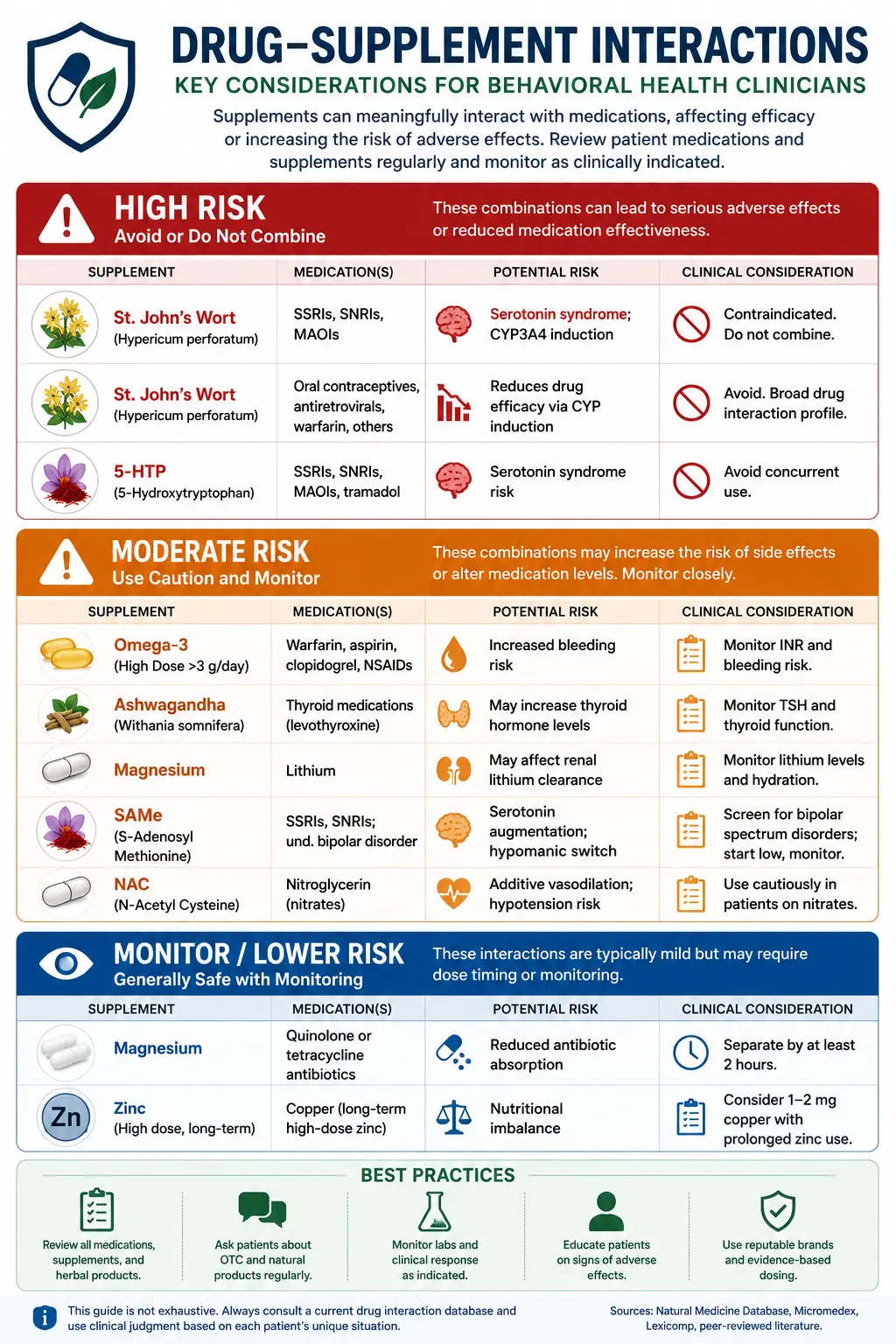
Drug-Supplement Interaction Reference Card
Many patients take supplements alongside antidepressants, mood stabilizers, and other psychiatric medications—but not all combinations are safe.
Download this free one-page clinical reference card to quickly identify common interactions involving SSRIs, SNRIs, lithium, anticoagulants, omega-3s, magnesium, SAMe, NAC, 5-HTP, ashwagandha, St. John's Wort, and more.
Practical Tips for Integrating Supplements into Treatment
- Order baseline 25(OH)D, B12, folate, zinc, and magnesium in patients where nutritional gaps are suspected. Targeted supplementation of documented deficiencies provides the strongest benefit. Screen for deficiencies first.
- Introduce adjuncts sequentially so you can attribute benefit or side effects accurately. Allow 4–6 weeks before assessing effect. Start one supplement at a time.
- Patient-purchased supplements are often significantly under-dosed. Discuss this directly and recommend products from manufacturers that use third-party testing (USP, NSF, or ConsumerLab verified). Use evidence-based doses.
- Record supplement use, dose, rationale, and monitoring plan in the clinical record. This protects the clinician and improves care coordination across providers. Document everything.
- Track symptom changes with validated tools (PHQ-9, GAD-7, DASS-21). If an adjunct isn’t helping after 6–8 weeks at a therapeutic dose, discontinue and reassess. Monitor outcomes systematically.
- Explain that supplements are not FDA-regulated in the same way as medications and that quality varies significantly. Encourage third-party tested products. Educate patients on quality.
- Nutritional status, medications, and health conditions change. What was appropriate 12 months ago may need adjustment.Revisit periodically.
Frequently Asked Questions About the Best Supplements for Mental Health
+What are the best vitamins for depression and anxiety?
+Does magnesium really help with anxiety?
+Is vitamin D deficiency linked to depression?
+Can supplements replace antidepressants or therapy?
+What is the best form of magnesium for anxiety?
+Does omega-3 fish oil help with depression?
+Are there supplements that interact with SSRIs?
+How do I choose a high-quality supplement for mental health?
Final Thoughts on Supplements for Mental Health
The evidence base for adjunctive nutraceuticals in behavioral health has matured considerably. Omega-3, L-methylfolate, vitamin D, magnesium, SAMe, and saffron are no longer fringe options — they are increasingly incorporated into clinical guidelines and recommended by integrative psychiatrists worldwide.
The most effective approach is systematic: screen for deficiencies, match the supplement to the patient’s presentation and biology, use therapeutic doses, and monitor outcomes. Combined with lifestyle interventions like exercise, light therapy, and mindfulness, these adjuncts give clinicians more tools to help patients who aren’t fully responding to conventional treatment — and give patients a sense of active participation in their own recovery.
As with any clinical decision, patient safety comes first. Know the interactions, document your recommendations, and revisit regularly.
How ICANotes Supports Clinicians Using Integrative Mental Health Approaches
Integrative mental health care requires clear, comprehensive documentation to ensure treatment plans reflect the full range of interventions — conventional and complementary. ICANotes makes it easy for clinicians to capture and track adjunctive strategies like nutraceutical use, lifestyle recommendations, and patient-reported outcomes. With customizable templates for progress notes, treatment plans, and intake assessments, you can document supplement regimens, monitor symptom changes, and coordinate care with other providers — all within a behavioral health-specific EHR.
ICANotes also supports evidence-based practice by enabling structured documentation of risk factors (e.g., nutrient deficiencies, sleep disruptions, or stress load) and tracking the impact of interventions like light therapy, mindfulness, or exercise over time. Whether you're incorporating omega-3s, recommending ashwagandha, or integrating mindfulness-based strategies, ICANotes gives you the clinical tools to document holistically, stay organized, and support better outcomes — without adding to your administrative burden.
Find out more by scheduling a demo or registering for a free 30-day trial (no credit card required).
Put Evidence Into Practice with ICANotes
Evidence-based care starts with evidence-based documentation. ICANotes helps behavioral health clinicians create comprehensive treatment plans, document medical necessity, track outcomes, and maintain compliant clinical records—without spending hours on paperwork.
Whether you're documenting depression, anxiety, medication management, supplement discussions, lifestyle interventions, or complex treatment plans, ICANotes streamlines clinical documentation so you can focus more time on patient care.
Join thousands of therapists, psychiatrists, psychiatric nurse practitioners, psychologists, and behavioral health organizations that trust ICANotes to simplify documentation and support quality patient care.
Start Your Free 30-Day Trial
No credit card required. Explore the behavioral health EHR trusted by thousands of mental health professionals.
Recent Posts


Dr. October Boyles
DNP, MSN, BSN, RN
Dr. October Boyles is a behavioral health expert and clinical leader with extensive expertise in nursing, compliance, and healthcare operations. With a Doctor of Nursing Practice (DNP) and advanced degrees in nursing, she specializes in evidence-based practices, EHR optimization, and improving outcomes in behavioral health settings. Dr. Boyles is passionate about empowering clinicians with the tools and strategies needed to deliver high-quality, patient-centered care.