Blog > Treatment Strategies > Postpartum Depression Symptoms, Signs, Screening, and Treatment
Postpartum Depression Symptoms, Signs, Screening, and Treatment: A Clinical Guide
Postpartum depression is a common but often misunderstood mood disorder that affects mothers, fathers, and the entire family system. This clinical guide reviews postpartum depression symptoms, explains what are signs of postpartum depression, differentiates PPD from baby blues and postpartum psychosis, and outlines key postpartum depression assessment and screening tools such as the EPDS and PDSS. Behavioral health clinicians will also learn how to treat postpartum depression using evidence-based approaches including CBT, IPT, medication, and collaborative care strategies to improve outcomes for parents and infants.
")
Last Updated: June 16, 2026

")
What You'll Learn
-
How to identify the most common postpartum depression symptoms, risk factors, and warning signs
-
Key differences between baby blues, postpartum depression, and postpartum psychosis
-
Questions to ask during a postpartum depression assessment to improve symptom disclosure
-
How to use screening tools such as the Edinburgh Postnatal Depression Scale (EPDS) and PDSS effectively
-
Critical safety concerns, including suicide risk and postpartum psychosis red flags
-
Evidence-based treatment planning strategies using CBT, IPT, behavioral activation, and family support interventions
-
Best practices for documenting assessment findings, treatment plans, progress, and medical necessity
-
Cultural and family-system considerations that may affect symptom presentation and treatment engagement
-
Strategies for supporting fathers, partners, and the broader family system
-
Practical steps for coordinating care with OB/GYNs, primary care providers, psychiatrists, and other members of the treatment team
Postpartum depression affects far more families than most people realize — and it rarely looks the way popular culture portrays it. It isn't always a mother weeping in a rocking chair. It can look like irritability, emotional numbness, relentless guilt, or a father quietly stopping at a bar on the way home from work.
For behavioral health clinicians, understanding the full presentation of postpartum depression — and knowing how to assess and treat it — is essential. This guide pulls together key clinical insights from a recent ICANotes webinar led by Diane Bigler, LCSW, a nationally recognized trainer in behavioral health, along with evidence-based recommendations for assessment and treatment.
What Is Postpartum Depression?
What Is Postpartum Depression?
Postpartum depression (PPD) is a mood disorder that occurs during pregnancy or after childbirth and causes persistent sadness, anxiety, irritability, guilt, and difficulty functioning. Unlike the baby blues, postpartum depression lasts longer than two weeks and often requires professional treatment.
Postpartum depression (PPD) is a mood disorder that can develop during pregnancy or after childbirth and affects a parent's emotions, thoughts, energy level, and ability to function. Unlike the "baby blues," which typically resolve within two weeks after delivery, postpartum depression persists longer and can significantly interfere with daily life, relationships, self-care, and infant bonding. Common postpartum depression symptoms include persistent sadness, anxiety, irritability, guilt, emotional numbness, fatigue, and difficulty concentrating. With early identification and appropriate treatment, most parents experience significant improvement and recovery.
What Are the Signs of Postpartum Depression?
The term "postpartum depression" is broadly recognized, but its actual presentation is highly variable. Before discussing what are signs of postpartum depression clinically, it's useful to distinguish it from two related but distinct conditions: the baby blues and postpartum psychosis.
Baby blues are common and typically self-resolving. They involve tearfulness, mood swings, and irritability in the first one to two weeks after birth and are largely driven by the dramatic hormonal shift following delivery.
Postpartum depression (PPD), by contrast, is a clinical mood disorder that persists beyond the first two weeks and significantly impairs functioning. Key postpartum depression symptoms include:
- Persistent sadness, hopelessness, or emotional emptiness
- Irritability, anger, or unexplained tearfulness
- Difficulty bonding with the baby
- Overwhelming guilt or beliefs of being a "bad" parent
- Fatigue that goes beyond ordinary new-parent sleep deprivation
- Loss of interest in previously enjoyed activities
- Withdrawal from friends and family
- Difficulty concentrating or making decisions
- Anxiety, including intrusive thoughts about the baby's safety
- In some cases, thoughts of self-harm or suicide

Reality Testing Remains Intact in Postpartum Depression
A parent experiencing postpartum depression may feel like a failure, struggle to get out of bed, or become overwhelmed by guilt and hopelessness. However, they still recognize that these thoughts and feelings are happening to them. Reality testing remains intact. This distinction is important because postpartum psychosis involves a loss of contact with reality and may include hallucinations, delusions, severe confusion, or impaired judgment.
Postpartum psychosis (PPP) is rare but constitutes a psychiatric emergency. It involves a loss of contact with reality: hallucinations (including command hallucinations), delusions — sometimes involving the baby — severe confusion, rapid mood swings, and disorganized behavior. PPP requires immediate medical and psychiatric intervention, with safety for the parent, baby, and family as the primary clinical concern.
Prior diagnoses of schizophrenia, bipolar disorder, or major depression significantly elevate risk for PPP and warrant especially close monitoring in the perinatal period.

Can Postpartum Depression Cause Anxiety?
Yes. Although postpartum depression is often associated with sadness and low mood, many parents experience significant anxiety symptoms as part of their condition. In some cases, anxiety may be more prominent than depression.
Common anxiety-related postpartum depression symptoms include:
- Excessive worry about the baby's safety or well-being
- Racing thoughts that are difficult to control
- Difficulty relaxing, even when the baby is safe and sleeping
- Intrusive thoughts that feel upsetting or frightening
- Physical symptoms such as muscle tension, restlessness, or a racing heart
- Constant feelings of being "on edge"
Because postpartum depression and anxiety frequently occur together, clinicians should assess for both conditions during screening and evaluation. Parents who present primarily with anxiety symptoms may still meet criteria for postpartum depression and benefit from treatment.

Free Clinical Download
Postpartum Depression Clinical Checklist
Assess, document, and treat postpartum depression with greater confidence. This practical checklist helps behavioral health clinicians identify symptoms, evaluate risk factors, screen for safety concerns, and develop evidence-based treatment plans.
- Identify postpartum depression symptoms and risk factors
- Differentiate PPD from baby blues and postpartum psychosis
- Support screening, treatment planning, and clinical documentation
PPD Is a Family Issue, Not Just a Maternal One
One of the most underappreciated aspects of postpartum depression is that it affects the entire family system — including fathers and partners.
Men can and do experience postpartum depression, though their presentation often differs from what we see in mothers. In fathers, PPD tends to show up as:
- Increased irritability, anger, or aggression
- Avoidance and withdrawal — including working longer hours
- Emotional detachment from the baby
- Emerging or escalating alcohol or substance use
Research suggests the highest-risk window for paternal PPD is when the baby is three to six months old. Critically, when a mother has PPD, up to 50% of partners also show depressive symptoms — making the partner's mental health an explicit clinical concern, not an afterthought.
For clinicians, this means assessment conversations should include fathers and partners directly, not just as informants about the mother's condition.
Postpartum Depression in Fathers and Partners
Postpartum depression is often discussed as a maternal mental health condition, but it can also affect fathers and partners. When one parent is struggling, the entire family system may feel the impact — and partners may experience their own depressive symptoms during the postpartum period.
Postpartum depression in fathers may not always look like sadness or tearfulness. Instead, it may present as irritability, anger, emotional withdrawal, avoidance, increased work hours, substance use, or feeling disconnected from the baby. Some fathers may also report sleep disruption, appetite changes, low motivation, or a sense of helplessness as they adjust to their new role.
Clinicians should consider asking fathers and partners direct questions about their mood, stress level, sleep, coping strategies, and connection with the baby. Including partners in postpartum depression assessment and treatment planning can help reduce isolation, strengthen family support, and improve outcomes for both the parent and infant.
Risk Factors for Postpartum Depression
Understanding which clients are at elevated risk helps clinicians prioritize early, proactive screening. Key risk factors include:
- Personal or family history of depression, anxiety, or bipolar disorder
- Low social support — isolation, geographic distance from family, or a partner with long work hours
- Complications during pregnancy or delivery, including emergency C-sections or traumatic birth experiences
- Severe sleep deprivation beyond the typical new-parent baseline
- Unplanned or unwanted pregnancy, particularly when the parent felt pressured to continue
- Recent major life changes, such as relocation during pregnancy
- History of trauma or adverse childhood experiences, especially those involving caretaking or attachment
- Financial stress or housing instability
Societal messaging also functions as a risk factor — the cultural narrative that mothers should feel instant joy and bond effortlessly, that "good" mothers sacrifice their own needs without struggle, and that postpartum distress should be endured quietly rather than treated. These messages deter help-seeking and can intensify a parent's shame and guilt.

Postpartum Depression Assessment: How to Open the Door
Before reaching for a standardized screening tool, experienced clinicians know that gently opening the door to conversation matters. A few targeted questions can signal to a new parent that their emotional experience is worth discussing:
- "How connected or emotionally bonded do you feel with your baby right now?"
- "In the past couple of weeks, how often have you felt sad, overwhelmed, or tearful without a clear reason?"
- "What kinds of thoughts do you notice about yourself as a parent — are they mostly supportive, or more self-critical?"
- "What has felt most emotionally difficult about the postpartum period for you so far?"
These questions apply equally to mothers and fathers and signal that the clinician is attending to both parents' experiences.
Don't overlook anxiety. Postpartum depression and anxiety frequently co-occur, and some parents present with anxiety as the dominant feature — racing thoughts, constant worry about the baby's safety, physical symptoms of tension — rather than sadness. Explicitly asking about anxious symptoms ensures this presentation isn't missed.
Cultural Considerations in Postpartum Depression Assessment
Cultural beliefs, family expectations, stigma, language barriers, and access to care can all shape how postpartum depression symptoms are experienced, described, and treated. For some parents, distress may be expressed through physical symptoms such as headaches, fatigue, body pain, or sleep disruption rather than through words like “sadness” or “depression.” Others may avoid disclosing symptoms because of shame, fear of judgment, concerns about being viewed as an unfit parent, or mistrust of the healthcare system.
Clinicians should use culturally responsive assessment strategies when screening for postpartum depression. This may include using validated translated screening tools, offering interpreter services, asking about cultural beliefs related to motherhood and help-seeking, and exploring the role of extended family, faith communities, immigration stress, financial barriers, and postpartum traditions.
A culturally responsive approach does not assume that all parents define distress, support, or recovery in the same way. Instead, it invites clients to describe their experience in their own words while helping them access safe, effective care. By addressing cultural and contextual factors directly, clinicians can reduce stigma, improve disclosure, and create treatment plans that feel more relevant and respectful to the families they serve.
Postpartum Depression Screening Tools
Standardized postpartum depression screening tools provide structured, validated data to supplement the clinical interview. The two most commonly used are:
Edinburgh Postnatal Depression Scale (EPDS)
The EPDS is the most widely used assessment for postpartum depression. It is a 10-item self-report tool that asks about the past seven days, covering mood, anxiety, guilt, and thoughts of self-harm. Scoring ranges from 0–30:
- Score ≥ 10: Possible depression — monitor closely
- Score ≥ 13: High risk; requires further clinical assessment
The EPDS is freely available online, takes under five minutes to complete, and has been validated across many languages and cultures. The self-harm item (Item 10) must always be reviewed immediately — any positive response warrants a direct safety assessment.
The EPDS is designed for use starting around two weeks postpartum, with optimal validity in the two-to-six-week window. It can be readministered to track progress over time.
Postpartum Depression Screening Scale (PDSS)
The PDSS is a longer 35-item tool that covers a broader range of domains: emotional lability, anxiety, sleep and eating disruption, and loss of self. It can be useful for clients who need more comprehensive structured assessment, and its time window extends somewhat beyond the EPDS's optimal range. However, some parents find its length burdensome, and many clinicians find the EPDS sufficient for most clinical contexts.
Key Principles for Postpartum Depression Screening
- Screenings are a starting point, not a diagnosis. A positive screen opens a clinical conversation; it doesn't conclude one.
- Pair screening scores with a clinical interview, collateral information, and assessment of functional impact.
- Screen early and repeatedly. Begin around two weeks postpartum and re-screen high-risk clients.
- The PHQ-9 can be used for ongoing symptom monitoring after the postpartum-specific screening window has passed.
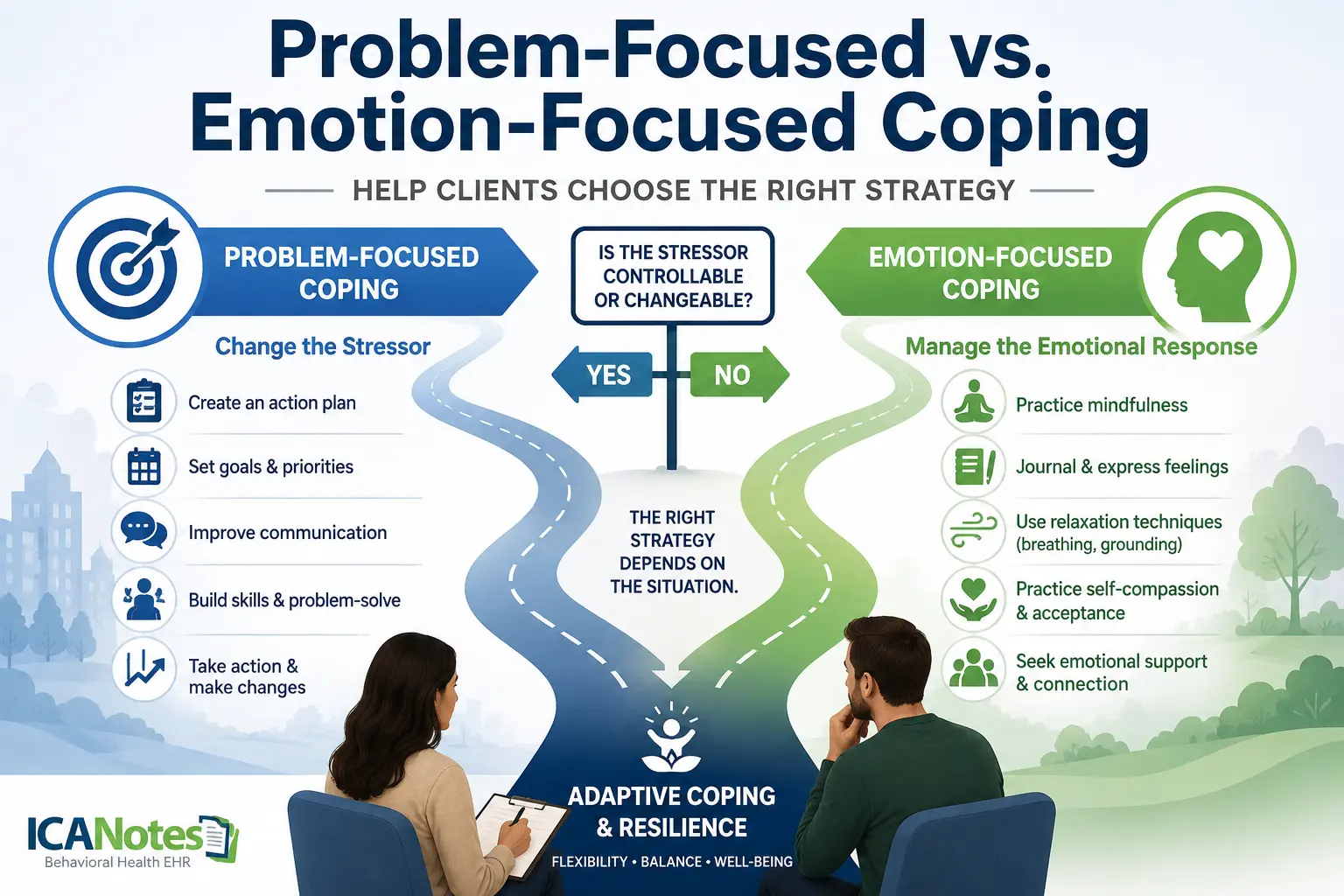
How to Treat Postpartum Depression: Evidence-Based Approaches
The evidence base for how to treat postpartum depression is well-established. Treatment should match symptom severity and be implemented promptly.
Psychotherapy: First-Line Treatment
Cognitive Behavioral Therapy (CBT) is one of the two most strongly supported interventions for PPD. Key targets include:
- Identifying and restructuring cognitive distortions (e.g., "I'm a terrible mother" → "I'm learning a new skill and it's okay to need help")
- Behavioral activation — reintroducing small, meaningful activities to rebuild routine, mastery, and pleasure
- Challenging "all-or-nothing" thinking around parenthood
Behavioral activation deserves particular emphasis. For parents who have withdrawn from daily life — avoiding friends, skipping self-care, disengaging from activities — structured, graduated activity scheduling can be a powerful early intervention.
Interpersonal Psychotherapy (IPT) is equally well-supported and particularly well-suited to the relational and transitional stressors of the postpartum period. IPT treatment targets include:
- Role transitions: Processing the shift into parenthood and grieving pre-parent identity
- Role disputes: Addressing conflict over childcare division, unmet expectations, or feeling excluded
- Grief and loss: Including losses tied to traumatic birth experiences
- Social support: Building and leveraging the parent's relational network
Other modalities with strong clinical rationale in the postpartum context include ACT (acceptance and values-based action), DBT skills for emotion regulation, solution-focused approaches for rapid symptom relief, and IFS for working with self-critical "parts." Trauma-focused approaches (TF-CBT, EMDR) are appropriate when birth trauma or prior adverse experiences are present.
Medication
Antidepressants — primarily SSRIs — are commonly prescribed for moderate to severe PPD. Breastfeeding compatibility should be part of the informed consent and treatment planning conversation.
Notably, zuranolone (Zurzuvae), a fast-acting 14-day oral medication specifically approved for PPD, represents a meaningful addition to the pharmacological toolkit. For severe cases, IV brexanolone (Zulresso) is also available. OB/GYNs frequently initiate antidepressants and then transfer ongoing psychiatric management to psychiatry — making warm handoffs and coordinated care essential.
Supportive and Complementary Approaches
- Peer support groups, including virtual options, reduce isolation and normalize the PPD experience
- Partner and family involvement — helping families reorganize around shared childcare, household tasks, and social support
- Psychoeducation: Helping parents understand that PPD is a medical condition, not a personal failure, and that early treatment significantly improves outcomes for both parent and child
Postpartum Depression Treatment Planning Guide
Treatment for postpartum depression should be individualized based on symptom severity, clinical presentation, risk factors, client preferences, and available support systems. The following table summarizes common evidence-based treatment approaches and their primary clinical applications.
Key Treatment Planning Considerations
When developing a postpartum depression treatment plan, clinicians should assess:
- Symptom severity and functional impairment
- Suicide risk and safety concerns
- Presence of anxiety, trauma, bipolar disorder, or substance use
- Quality of social and family support
- Breastfeeding considerations when discussing medication options
- Cultural beliefs and barriers to care
- Parent-infant bonding concerns
- Client preferences regarding treatment approaches
Early intervention and coordinated care among behavioral health providers, OB/GYNs, pediatricians, and psychiatric prescribers can significantly improve outcomes for both parents and infants.
How Long Does Postpartum Depression Last?
The duration of postpartum depression varies from person to person. Symptoms may begin during pregnancy, within the first few weeks after childbirth, or anytime during the first year postpartum.
Without treatment, postpartum depression can persist for many months and may negatively affect parental functioning, relationships, and infant development. Fortunately, most people improve significantly with appropriate treatment and support.
Factors that may influence recovery include:
- Symptom severity
- Access to mental health treatment
- Social and family support
- Sleep quality
- Co-occurring mental health conditions
- Early identification and intervention
Because symptoms can emerge or worsen over time, ongoing screening and follow-up are important, particularly for individuals with known risk factors.

Barriers to Seeking Help — and How Clinicians Can Address Them
Many parents who need support don't ask for it. Common barriers include stigma, cultural expectations about "bouncing back," fear of judgment, not knowing who to ask, and the belief that struggling makes them a bad parent.
One practical clinical strategy: present the list of common barriers directly to clients and invite them to identify which resonate. This can open conversation, reduce shame, and help the clinician tailor their approach to the individual's specific obstacles.
The Collaborative Care Model
Clinicians working in behavioral health don't work in isolation. Effective PPD care increasingly depends on coordination across the care team — including OB/GYNs, pediatricians, and psychiatry. Many new parents encounter the healthcare system most frequently through obstetric and pediatric visits, making those touchpoints critical opportunities for screening and warm referral.
As Dr. Vivian Burk (UCLA) and colleagues have noted, rising maternal mortality, morbidity, and suicide rates reflect a systemic gap in access to care — and addressing it requires collaborative infrastructure, not individual heroism.
When to Seek Emergency Help
While most cases of postpartum depression can be treated successfully through outpatient care, some symptoms require immediate medical attention.
Seek emergency psychiatric evaluation if a parent experiences:
- Hallucinations (hearing or seeing things others do not)
- Delusions or false beliefs, particularly involving the baby
- Severe confusion or disorientation
- Rapid mood swings accompanied by impaired judgment
- Thoughts of harming themselves
- Thoughts of harming the baby
- Loss of contact with reality
These symptoms may indicate postpartum psychosis, a rare but serious psychiatric emergency that requires immediate intervention to protect the safety of both parent and child.
How ICANotes Supports Postpartum Depression Assessment and Documentation
Accurate assessment, treatment planning, and documentation are essential when working with clients experiencing postpartum depression. Clinicians must be able to identify symptoms, assess risk factors, document medical necessity, track treatment progress, and maintain compliance with payer and regulatory requirements.
The ICANotes Behavioral Health EHR helps streamline this process by providing specialty-specific documentation tools designed for mental and behavioral health providers. During postpartum depression assessments, clinicians can efficiently document presenting symptoms, mood changes, anxiety, sleep disturbances, bonding concerns, psychosocial stressors, and relevant risk factors. Structured templates help ensure that important clinical information is captured consistently while reducing the time spent on documentation.
When developing a treatment plan, clinicians can document evidence-based interventions such as Cognitive Behavioral Therapy (CBT), Interpersonal Psychotherapy (IPT), behavioral activation, psychoeducation, family support strategies, and medication management. Progress notes can be completed quickly while still reflecting clinical decision-making, treatment goals, symptom changes, and ongoing risk assessment.
ICANotes also supports collaboration across the continuum of care by maintaining comprehensive clinical records that can be shared, when appropriate, with psychiatrists, primary care providers, OB/GYNs, and other members of the treatment team. This can be particularly valuable when managing postpartum depression, where coordinated care often leads to better outcomes for both parents and infants.
By simplifying documentation and helping clinicians maintain thorough, clinically relevant records, ICANotes allows providers to spend less time typing and more time focusing on patient care.
Postpartum Depression Resources for Clinicians and Clients
Explore screening tools, support organizations, educational resources, and self-help workbooks that can help clinicians, parents, and families better understand and navigate postpartum depression and perinatal mental health challenges.
Edinburgh Postnatal Depression Scale (EPDS)
Widely used postpartum depression screening tool that helps clinicians identify depressive symptoms during pregnancy and the postpartum period.
Postpartum Depression Screening Scale (PDSS)
Screening resource designed to help identify postpartum depression symptoms and support early intervention efforts.
Postpartum Support International
Leading nonprofit organization providing education, support groups, referrals, and resources for perinatal mental health.
Alexis Joy Foundation
Advocacy and support organization focused on maternal mental health awareness, education, and access to care.
Resources for Fathers (Maternal Mental Health Leadership Alliance)
Educational resources from the Maternal Mental Health Leadership Alliance addressing paternal postpartum mental health and family support.
Postpartum Men
Resource hub dedicated to paternal postpartum depression, anxiety, adjustment challenges, and family wellness.
Pregnancy & Postpartum Mental Health Toolkit (VA)
Comprehensive clinical toolkit covering screening, treatment, risk factors, and care considerations during pregnancy and postpartum.
CBT Workbook for Postpartum Depression (HeretoHelp BC)
Cognitive behavioral therapy self-help workbook designed to help individuals manage depression during pregnancy and after childbirth.
Gaining Control of Your Life After Having a Baby (Self-Help Workbook)
Evidence-informed self-help workbook offering practical strategies for managing postpartum depression and supporting recovery.
Frequently Asked Questions About Postpartum Depression
Recent Posts


Diane Bigler
LCSW, LSCSW
About the Author
Diane Bigler, LCSW, LSCSW, is a Licensed Clinical Social Worker in Missouri and Kansas with over 25 years of experience in the mental health field. She has held clinical positions as an outpatient and in-home therapist and clinical supervisor in diverse settings. Diane was an Adjunct Professor of Social Work for 10 years at The University of Kansas, School of Social Welfare and a Field Liaison and Field Instructor. She has also held administrative positions as a Program Director and Coordinator. Diane is a popular local and national trainer on a wide variety of mental health and workplace development topics for clinicians and corporations and has facilitated over 500 training courses in the last few years. Visit her website http://www.