Blog > Practice Management > Therapy Intake Questions: A Clinician's Guide
Therapy Intake: A Clinician's Guide for Mental Health, Counseling & Psychiatry
Therapy intake questions, process steps, and documentation examples for clinicians conducting mental health, counseling, and psychiatry intakes. This guide includes a structured checklist, what to ask during an intake session, and a sample therapy intake note to support accurate, efficient documentation.

Last Updated: April 28, 2026

")
What You'll Learn
- A structured set of therapy intake questions to ask, organized by category
- How to conduct an effective intake session without losing clinical flow
- What to include in therapy intake documentation for compliance and clarity
- A sample therapy intake note to guide your own documentation
- Key differences between mental health, counseling, and psychiatry intakes
- What clients can expect during an intake (and how to set the right tone)
- Common therapy intake mistakes — and how to avoid them
The therapy intake session sets the foundation for everything that follows — from diagnosis and treatment planning to client engagement and continuity of care. But for many clinicians, the challenge isn’t knowing that the intake matters — it’s knowing exactly what to ask, what to document, and how to structure the conversation without losing clinical flow.
This guide brings those elements together in one place. You’ll find a structured set of therapy intake questions, organized by category, along with practical guidance on conducting the intake session, documenting it effectively, and avoiding common mistakes. Whether you’re conducting mental health, counseling, or psychiatry intakes, this resource is designed to support both clinical thoroughness and efficiency.
What is a Therapy Intake?
A therapy intake is the initial appointment between a mental health provider and a new client. It serves as the foundation for building a therapeutic relationship and gathering essential clinical information. The goal is to understand why the client is seeking help, assess their current mental health status, and begin formulating an appropriate treatment plan.
In a mental health intake, clinicians typically explore presenting concerns, personal and family history, medical background, and psychosocial factors. This session often includes a mental status exam (MSE) to evaluate mood, affect, thought processes, orientation, and other cognitive functions.
A counseling intake may place more emphasis on emotional experiences, relationship dynamics, and personal goals. It also gives the therapist a chance to introduce their therapeutic approach and begin building rapport.
For clients pursuing psychiatric care, the psychiatry intake includes additional focus on diagnostic clarification, medication history, and potential treatment with psychopharmacology. Psychiatrists or
Free download
Therapy Intake Questions Checklist
A practical, ready-to-use checklist covering the 8 core categories of therapy intake questions — from presenting concern and symptoms to risk, psychosocial context, and goals. Use it as a flexible guide to structure intake sessions and ensure nothing important is missed.
- Organized by clinically relevant intake categories
- Supports thorough, structured intake sessions
- Helps guide conversation without losing flow
- Works for therapy, counseling, and psychiatry intakes
Instant access.
psychiatric nurse practitioners often use this session to determine whether medication, therapy, or a combination is most appropriate.
Regardless of discipline, the intake process is not just about collecting data — it’s about creating a safe, supportive space where clients feel heard and respected. A well-executed intake sets the tone for all future sessions and helps ensure clinical effectiveness, risk mitigation, and regulatory compliance.
Mental Health vs. Counseling vs. Psychiatry Intake: Key Differences
Although the three intake types share a common foundation, each emphasizes different clinical priorities. The table below summarizes how mental health, counseling, and psychiatry intakes typically differ in scope, focus, and follow-up — useful both for clinicians refining their own intake workflow and for clients trying to understand what their first session will involve.
| Element | Mental Health Intake | Counseling Intake | Psychiatry Intake |
|---|---|---|---|
| Primary focus | Comprehensive clinical baseline — presenting concerns, history, functioning, and risk. | Therapeutic alliance, emotional context, and collaborative goal-setting. | Diagnostic clarification and the role of medication in care. |
| Typical duration | 60–90 minutes | 50–60 minutes | 60–90 minutes (longer for complex presentations) |
| Conducted by | Licensed therapists, clinical social workers, and licensed mental health counselors. | Licensed professional counselors, marriage and family therapists, and licensed therapists. | Psychiatrists, psychiatric nurse practitioners, and physician assistants. |
| Key questions |
|
|
|
| Common assessments |
|
|
|
| Documentation focus | Presenting concerns, history of present illness, MSE, risk assessment, working diagnosis, and initial treatment plan. | Presenting concerns, psychosocial context, agreed-upon goals, and the therapeutic approach. | HPI, psychiatric ROS, MSE, diagnostic formulation, medication plan, and risk. |
| Common next steps | Begin scheduled therapy sessions, refine the treatment plan, refer for psychiatric or medical evaluation if indicated. | Schedule recurring counseling sessions, agree on an initial focus, share supportive resources. | Initiate or adjust medication, order labs if needed, schedule a follow-up in 2–4 weeks, coordinate with the therapist. |
Regardless of which intake type you're conducting, the underlying goals are the same: build trust, gather the clinical information needed to inform care, identify safety concerns, and establish a treatment direction the client is engaged with.
Preparing for the Intake Session
Laying the groundwork before a therapy intake session helps set the tone for a smoother, more productive experience — for both you and your client. A well-prepared mental health intake shows professionalism, builds trust, and creates space for deeper connection and insight once the session begins.
Below are key preparation steps to take before the appointment:
1. Organize Intake Paperwork in Advance
Therapy, counseling, and psychiatry intake sessions require a variety of forms, including informed consent, HIPAA privacy notices, screening tools, and medical or mental health history questionnaires. Preparing this paperwork ahead of time ensures the session starts on time and with fewer disruptions.
Many mental health providers also include a personalized welcome letter that introduces their therapeutic approach, credentials, practice policies, and contact information. If you use an EHR with a secure patient portal, consider sending these documents electronically for clients to complete prior to the appointment. This not only streamlines the intake process but also helps clients feel more prepared.
2. Review the Client’s Background Information
Before the intake appointment, take time to review any available background information. This may include prior medical or psychiatric records, intake forms submitted through your portal, or details included in the client’s appointment request.
Gaining context in advance can help you approach the counseling intake session with empathy and direction, especially if the client is reluctant to open up. If you're working within a psychiatry intake, having a clear picture of past diagnoses or medications can also guide more efficient evaluation.
3. Prepare Thoughtful Intake Questions
While some clients will come in ready to talk, others may need gentle prompting. Having a list of thoughtful, open-ended questions ready can make a big difference. Cover essential areas such as:
-
Presenting symptoms and duration
-
Triggers or stressors
-
Safety concerns (e.g., self-harm or suicidal ideation)
-
Client goals for therapy or treatment
-
Relevant items from their intake form
Whether you’re conducting a mental health, counseling, or psychiatry intake, these questions help ensure you collect clinically meaningful information while building rapport from the very first session.
Therapy Intake Questions to Ask
The questions you ask during a therapy intake do more than gather data — they help clients feel heard, surface clinically meaningful information, and shape the direction of treatment. The list below organizes commonly used intake questions by category. You won't ask all of them in a single session; instead, use them as a flexible reference, prioritizing the areas most relevant to your client's presenting concerns and your discipline.
The diagram below shows the 8 core categories of therapy intake questions, providing a simple framework you can follow during any intake session.

Presenting concern
- What brings you in today?
- How long has this been going on, and what made you decide to seek help now?
- Has anything specific happened recently that's made things harder?
- How is this affecting your daily life — work, school, relationships, sleep?
- In your own words, what would you most like to address first?
Symptoms, history, and functioning
- How would you describe your mood lately, in general?
- Are you experiencing changes in sleep, appetite, energy, or concentration?
- Have you had any thoughts that worry you — racing thoughts, intrusive thoughts, or anything else?
- Have you experienced anything like this before? When?
- Is there a history of mental health concerns in your family?
Risk and safety
- Have you had any thoughts of harming yourself or ending your life — recently or in the past?
- Have you ever acted on those thoughts, or thought about how you might?
- Are you currently safe at home, in your relationships, and in your work or school environment?
- Do you have access to firearms, medications in large quantities, or other means of harm?
- Have you had any thoughts of harming someone else?
Medical, medication, and substance use history
- What medical conditions do you have, and what medications are you currently taking?
- Have you taken any psychiatric medications in the past? What worked or didn't work?
- Do you have any drug allergies or sensitivities?
- How would you describe your use of alcohol, tobacco, caffeine, or other substances?
- How much sleep are you typically getting, and how restful is it?
Psychosocial context and supports
- Who lives at home with you, and how would you describe those relationships?
- Who do you turn to when things are hard?
- How are things at work or school right now?
- Are there cultural, religious, or community values that are important to you and that you'd want me to understand?
- Have you experienced significant losses, transitions, or stressors recently?
Strengths, coping, and resilience
- When you've gotten through hard times in the past, what has helped?
- What are some things you do that bring you a sense of calm or grounding?
- What are you good at, or proud of, that you might not bring up otherwise?
- Who or what in your life feels stable or supportive right now?
Prior treatment experiences
- Have you worked with a therapist, counselor, or psychiatrist before?
- What was helpful or unhelpful about that experience?
- Is there anything you'd like to do differently this time?
- Are you currently working with any other providers we should coordinate with?
Goals and motivation
- What would success look like for you over the next few months?
- If we worked together for six months and things were better, what would be different?
- Are there changes you're hoping to see in your relationships, your work, or how you feel day-to-day?
- On a scale of 1 to 10, how ready do you feel to make changes right now?
Pro tip — pacing the questions
The strongest intakes balance structured inquiry with conversational flow. Open with broad, open-ended questions, narrow into specifics as the client shares, and always close with goals and motivation. If a sensitive area surfaces unexpectedly, follow it — you can return to your checklist after.
Mental Health Intake Questions: What to Ask and Observe
Once your client arrives, the mental health intake officially begins. This session is your opportunity to gather clinical insights, observe client behavior, and begin building a therapeutic alliance. Whether you're conducting a therapy intake for general mental health concerns or a more targeted counseling intake, the questions you ask, and the way you listen, set the stage for effective care.
Ask Open-Ended Questions
The most effective intakes strike a balance between structured inquiry and empathetic conversation. Start with open-ended questions that invite clients to share their experiences in their own words. For example:
-
"Can you tell me what brought you in today?"
-
"What kinds of things have you been struggling with lately?"
-
"How are these challenges affecting your daily life?"
These types of questions help you learn about the client’s concerns without overwhelming them during the first visit. Letting them speak freely can also ease anxiety and help them feel more comfortable opening up.

Assess Symptom Patterns and Risk
As the session progresses, transition into more targeted questions about symptoms, duration, and impact. Explore areas such as:
-
Mood, anxiety, or trauma-related symptoms
-
Sleep and appetite changes
-
Concentration and energy levels
-
Substance use history
-
Experiences of loss or grief
It’s also critical to assess risk factors during the intake. Ask whether the client has experienced thoughts of self-harm or suicidal ideation. Depending on their response, follow up with more detailed safety assessments and create a safety plan if necessary.

Observe Client Behavior and Affect
Beyond verbal responses, pay close attention to nonverbal cues. A mental health intake offers a unique opportunity to assess the client's presentation, including:
-
Mood and affect (Are they congruent?)
-
Speech patterns (Paced? Pressured? Hesitant?)
-
Eye contact and body language
-
Orientation to person, place, and time
These observations often form the basis of the mental status exam (MSE) and contribute to diagnostic impressions and treatment planning. Note any discrepancies between what the client says and how they present.
Discuss Client Goals
Toward the end of the intake, explore what the client hopes to achieve through therapy, counseling, or psychiatry. Understanding their goals helps align your clinical approach and sets expectations for future sessions.
You might ask:
-
"What would you like to get out of therapy?"
-
"Are there changes you’re hoping to see in your life or relationships?"
-
"Have you worked with a therapist, counselor, or psychiatrist before? What was that like?"
Clarifying these goals helps you create a collaborative treatment plan and shows clients you're invested in their progress from the very beginning.
The therapy intake process follows a structured sequence — from collecting pre-session information to documenting findings and developing a treatment plan. The diagram below outlines the key steps in a typical intake workflow, helping clinicians stay organized while maintaining a natural, client-centered conversation.
Pre-Intake Forms
Collect demographics, history, consent forms, and screening information before the session.
Intake Session
Ask structured therapy intake questions while building rapport and understanding the client’s goals.
Assessment
Review symptoms, history, risk, functioning, strengths, and relevant clinical impressions.
Documentation
Document the intake note, MSE, risk assessment, diagnosis, and initial plan clearly.
Treatment Plan
Translate intake findings into initial goals, interventions, referrals, and next steps.
Therapy Intake Form: What to Include
A well-designed therapy intake form does most of the information-gathering before the client ever sits down with you, freeing the session itself for clinical conversation. A strong intake form is comprehensive enough to support diagnosis and treatment planning, but structured so it doesn't overwhelm clients on day one.
At a minimum, your therapy intake form should capture:
- Client demographics, contact information, and emergency contact.
- Insurance information and consent to bill.
- Presenting concerns and reason for seeking treatment.
- Mental health history, including prior diagnoses and treatment.
- Current medications, dosages, prescribers, and known drug allergies.
- Substance use history.
- Medical history and primary care provider.
- Family psychiatric history.
- Psychosocial history — relationships, work or school, supports.
- Cultural, spiritual, and identity factors the client wants the clinician to know.
- Symptom checklist or screening tools (e.g., PHQ-9, GAD-7) when appropriate.
- Informed consent, HIPAA acknowledgment, and telehealth consent (if applicable).
When clients complete the form through a secure patient portal before the session, you can review their responses in advance, prepare follow-up questions, and use the appointment time for the work that actually requires the two of you to be in the room together. In ICANotes, intake data submitted through the portal automatically pulls into the initial assessment, so clinicians can review and edit rather than re-enter.
Free download
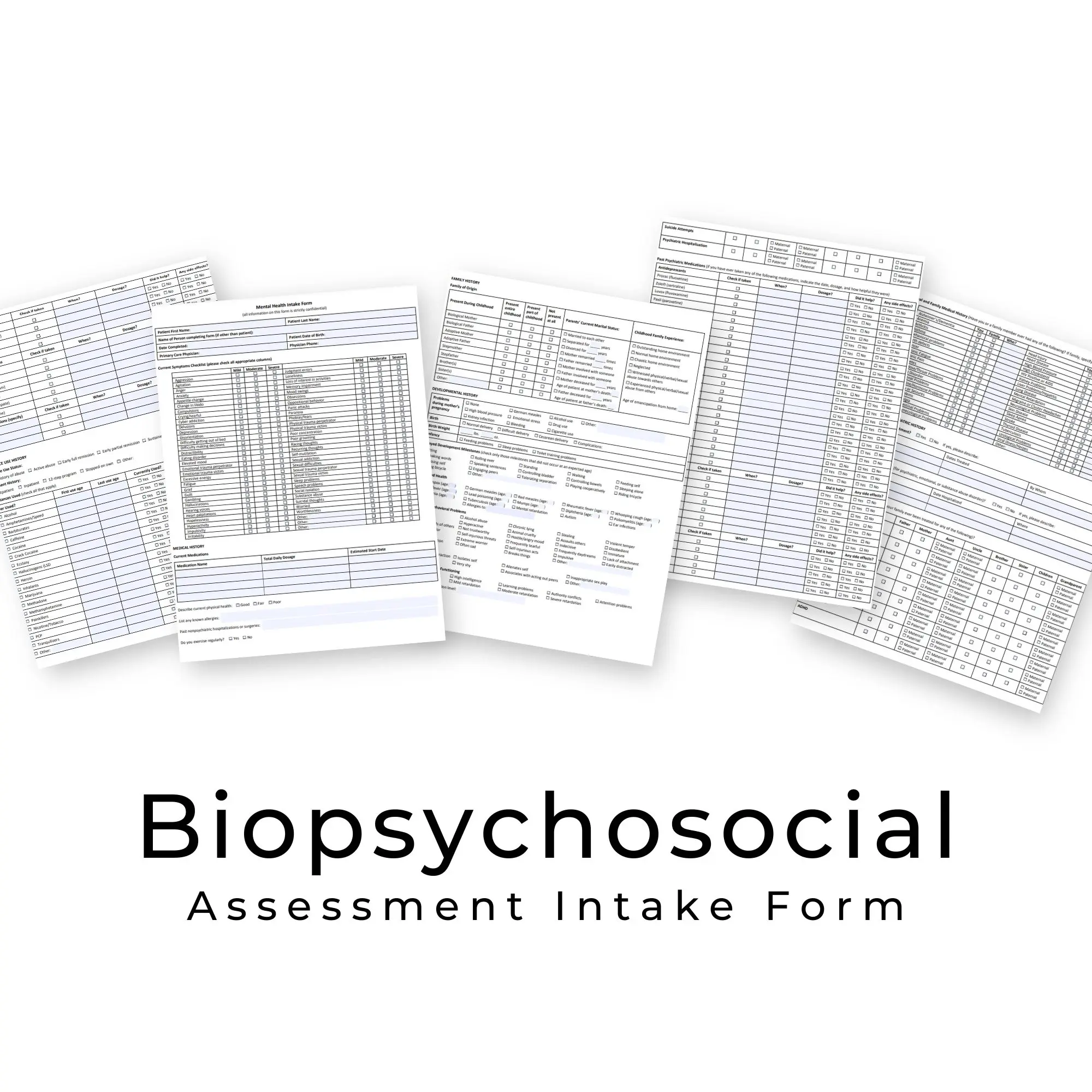
Fillable Biopsychosocial Intake Form
A ready-to-use intake form designed for behavioral health: mental health symptom checklist, medical and psychiatric history, substance use and medication tracking, developmental and psychosocial history, and cultural and spiritual context.
Counseling Intake Questions and Considerations
A counseling intake is more than a clinical information-gathering exercise, it’s the first step in forming a therapeutic alliance. While it shares structural elements with other types of mental health intake sessions, counseling intakes often place greater emphasis on the emotional experience of the client, rapport-building, and collaborative goal setting.
Here are key considerations when conducting a counseling-focused therapy intake:
Prioritize Emotional Safety
For many clients, the counseling intake may be their first time talking openly about painful or deeply personal issues. Creating a safe, supportive environment is essential. Use affirming language, nonjudgmental listening, and empathetic body language to build trust early.
Many counselors open the session with a warm acknowledgment, such as:
“I know the first session can feel a little intimidating. I really appreciate you being here and sharing what you’re comfortable with at your own pace.”
This helps ease anxiety and sets a collaborative tone.
Explore Psychosocial Context
A comprehensive counseling intake should cover more than symptom checklists, it should explore the client’s environment and support system. Consider asking about:
-
Current relationships and family dynamics
-
Social supports and sources of stress
-
Cultural, spiritual, or community affiliations
-
Work, school, or caregiving responsibilities
These insights are critical for tailoring your therapeutic approach and identifying potential barriers to treatment.
Assess Readiness and Motivation
Understanding where your client stands in terms of readiness for change can guide your treatment plan and help you match interventions appropriately. Motivational interviewing techniques, such as asking what prompted them to seek help now, can yield meaningful responses and uncover internal motivations.
Ask questions like:
-
“What led you to consider counseling at this time?”
-
“What changes would you like to see in your life?”
-
“Have you tried anything in the past that helped?”
These responses can help shape a collaborative treatment plan and give insight into the client’s coping strategies and resilience.
Acknowledge Past Counseling Experiences
If the client has participated in therapy before, take time to understand what worked and what didn’t. This helps you avoid repeating unhelpful patterns and lets the client feel heard.
Sample prompts include:
-
“Have you worked with a therapist or counselor before?”
-
“What was helpful or unhelpful about that experience?”
-
“Is there anything you’d like to do differently this time?”
Tailoring the counseling intake to the individual promotes client autonomy and fosters stronger engagement in the therapeutic process.

Psychiatry Intake Questions: What to Cover
A psychiatry intake is a specialized form of mental health intake that focuses on both the psychological and biological factors influencing a client’s well-being. While it shares core elements with a general therapy intake, psychiatry intakes also require a deeper exploration of medical history, diagnostic clarification, and potential treatment with psychopharmacology.
Here are the essential areas to address during a psychiatry intake:
Comprehensive Medical and Psychiatric History
Begin by reviewing the client’s past and current diagnoses, any hospitalizations, and significant psychiatric events. Explore their medication history in detail, including:
-
Current medications, dosages, and adherence
-
Past psychiatric medications and reasons for discontinuation
-
Side effects experienced and tolerability
-
Known drug allergies or interactions
This information provides the foundation for safe prescribing and helps identify patterns in medication response.
Diagnostic Assessment
A psychiatry intake often includes a more structured diagnostic evaluation than a counseling intake. This may involve:
-
Detailed symptom exploration (onset, severity, triggers)
-
Use of standardized screening tools
-
Assessment of co-occurring mental health and medical conditions
-
Differentiation between psychiatric and medical causes of symptoms
Your assessment should also include a mental status exam (MSE) to evaluate cognitive functioning, affect, thought processes, and insight.
Substance Use and Lifestyle Factors
Because medication effectiveness and safety can be affected by lifestyle habits, discuss:
-
Substance use (alcohol, recreational drugs, nicotine)
-
Caffeine intake
-
Sleep hygiene
-
Nutrition and exercise patterns
These factors can influence medication metabolism, symptom presentation, and overall treatment success.
Risk Assessment
As with any mental health intake, it’s essential to evaluate safety concerns, including:
-
Suicidal ideation or self-harm behaviors
-
Risk of harm to others
-
Access to means (e.g., firearms, medications)
If risk factors are identified, create a clear safety plan and document it thoroughly.
Treatment Planning and Education
Conclude the psychiatry intake by discussing treatment options. This may include:
-
Initiating or adjusting medication
-
Recommending psychotherapy or counseling
-
Suggesting lab work or physical exams to rule out medical causes
-
Providing psychoeducation about diagnosis, prognosis, and medication use
Encourage client questions and collaboration in the decision-making process to promote adherence and trust.
Common Therapy Intake Mistakes to Avoid
Whether you’re conducting a therapy intake, a mental health intake, a counseling intake, or a psychiatry intake, the first session sets the tone for your client’s entire treatment experience. Even skilled clinicians can fall into habits that reduce the effectiveness of the intake process. Being aware of these common pitfalls, and taking steps to avoid them, can help you start every client relationship on the right foot.
1. Rushing Through the Process
The intake is not just a formality, it’s the foundation of your clinical work. Moving too quickly can leave clients feeling unheard and can cause you to miss important information about symptoms, history, or risk factors. Allow enough time for clients to share their story and for you to ask follow-up questions.
2. Over-Reliance on Forms and Checklists
While intake forms, consent documents, and screening tools are essential, relying solely on paperwork can make the session feel impersonal. Use these tools as a guide, but prioritize active listening and conversational rapport-building.
3. Using Overly Clinical or Technical Language
Clients may be unfamiliar with clinical terminology, especially during a first session when they may already feel anxious. Strive to explain terms and processes in plain language. This is especially important in psychiatry intakes, where medication and diagnostic discussions can quickly become complex.
4. Skipping Risk Assessment Questions
Even if the client appears stable, you should never skip questions about self-harm, suicidal ideation, or other safety concerns. Failing to address these can put both the client and clinician at risk. Risk assessment is a critical part of every mental health intake, regardless of the presenting issue.
5. Neglecting to Explore Client Goals
An intake that focuses only on symptoms and history, without exploring what the client hopes to gain from treatment, can make therapy feel disconnected from their personal needs. Discussing goals early helps align your treatment plan with the client’s expectations.
6. Not Documenting Thoroughly
Accurate and complete documentation isn’t just about compliance — it ensures continuity of care, supports collaboration with other providers, and protects you legally. Whether you’re conducting a counseling intake or a psychiatry intake, note key observations, client statements, and your clinical impressions.
Tips for Creating a Supportive Intake Environment
A well-run therapy intake isn’t just about collecting information — it’s about setting the tone for a safe, trusting, and collaborative therapeutic relationship. Whether you’re conducting a mental health intake, counseling intake, or psychiatry intake, the environment you create plays a powerful role in how open and comfortable clients will feel during your first meeting.
1. Start with Warm, Welcoming Communication
Begin the session by greeting the client warmly and expressing appreciation for their willingness to meet. A simple acknowledgment, such as, “I’m glad you’re here today, and I want you to feel free to share at your own pace,” can help reduce anxiety and establish rapport.
2. Set Clear Expectations
Clients often feel more comfortable when they know what to expect from the intake process. Outline the session structure, explain the purpose of your questions, and clarify how the information will be used. In psychiatry intakes, this may include describing the role of medication evaluation alongside therapeutic support.
3. Create a Comfortable Physical or Virtual Space
If meeting in person, ensure the environment is quiet, private, and free from distractions. If the intake is conducted via telehealth, test your technology in advance and encourage the client to choose a private, comfortable space for the session.
4. Demonstrate Cultural Humility
Clients bring unique cultural, religious, and personal values into the therapy room. Show respect and openness to their perspectives. Incorporating culturally sensitive language during the mental health intake can enhance trust and improve treatment engagement.
5. Balance Structure with Flexibility
While it’s important to cover essential clinical topics, be ready to adapt your approach if the client brings up something significant. Flexibility allows for deeper connection and signals that you value the client’s input as much as your own clinical agenda.
6. Affirm Strengths and Resilience
During the counseling intake, take time to recognize and affirm the strengths the client has already demonstrated, whether it’s seeking help, using coping strategies, or maintaining supportive relationships. Positive reinforcement can boost client confidence and engagement from the very first session.
Therapy Intake Notes: Documentation and Compliance
Accurate, thorough documentation is a critical part of every therapy intake, whether you’re conducting a mental health intake, counseling intake, or psychiatry intake. Beyond keeping a record of client information, well-documented intake notes ensure continuity of care, support insurance reimbursement, and protect you in the event of audits or legal inquiries.
1. Capture All Required Clinical Elements
Your intake documentation should include:
-
Client demographic information and contact details
-
Presenting concerns and history of the problem
-
Medical, psychiatric, and psychosocial history
-
Current medications, allergies, and prior treatments
-
Observations from the mental status exam (MSE)
-
Risk assessments (suicidality, self-harm, harm to others)
-
Client treatment goals and agreed-upon next steps
Completing these sections in detail not only meets clinical standards but also supports compliance with payer requirements and professional ethics.
2. Document in Real Time When Possible
Recording intake details promptly, ideally during or immediately after the session, helps ensure accuracy and completeness. Waiting too long increases the risk of omitting important client statements, observations, or your own clinical impressions. Using a specialty-specific behavioral health EHR like ICANotes can help you document in real time, and significantly reduces the time spent on documentation without compromising quality.
3. Maintain Compliance with Privacy Regulations
All intake documentation must comply with HIPAA and, if applicable, 42 CFR Part 2 confidentiality rules for substance use treatment. This includes securely storing electronic health records and limiting access to authorized personnel.
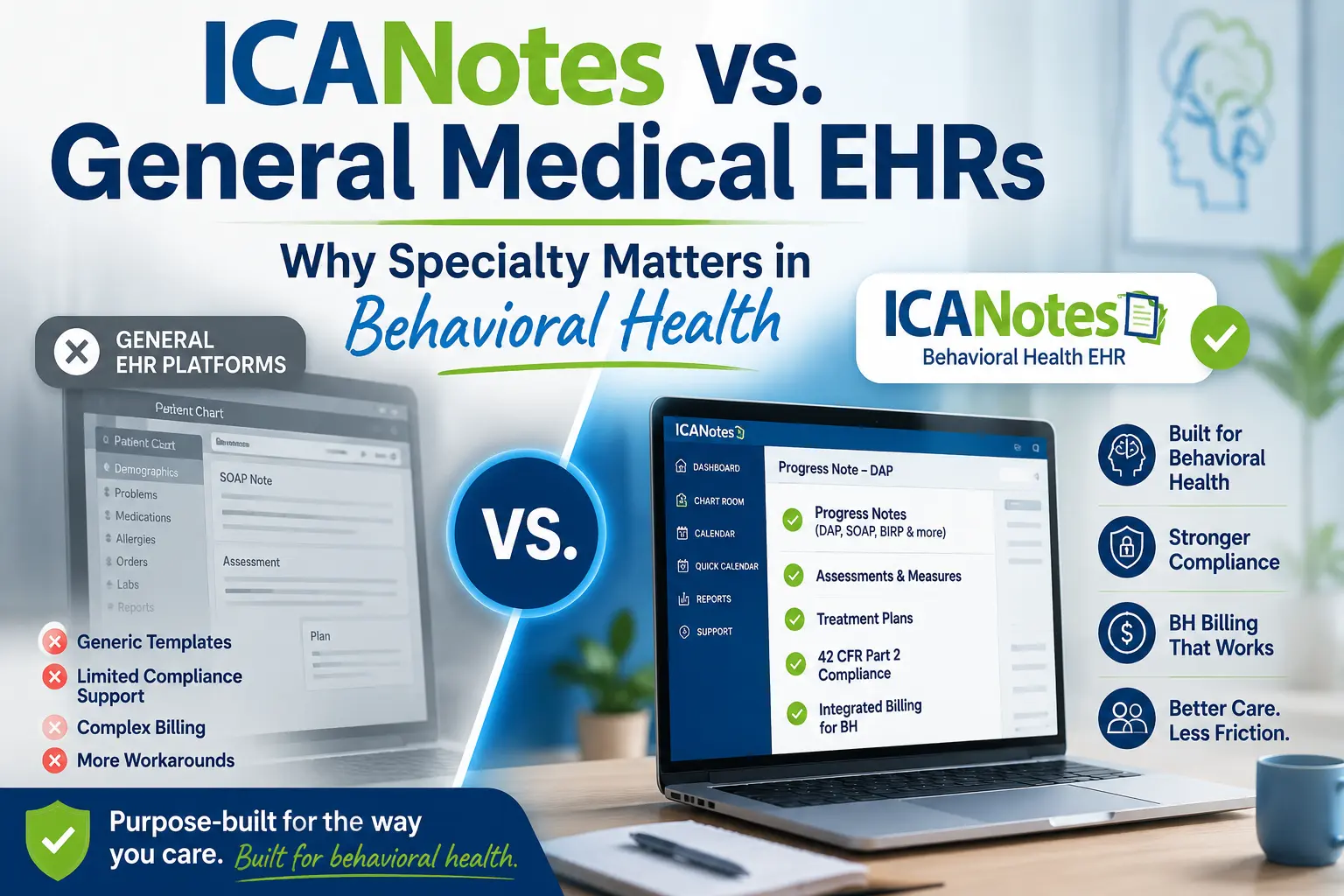
4. Leverage Your EHR for Efficiency
Using an EHR with behavioral health–specific intake templates can streamline the process, reduce administrative burden, and improve note quality. For example, ICANotes offers structured intake templates that prompt for all required clinical elements while allowing you to personalize the note for each client. Secure patient portal features can also collect intake forms ahead of time, saving valuable session time for meaningful discussion. In ICANotes, the client enters all of the intake information via the portal prior to the intake session, and the data automatically pulls into the initial assessment for review and editing by the clinician.
5. Support Collaboration and Care Coordination
Intake notes are often shared, either in full or in summary, with other members of a client’s care team. Writing clear, concise, and well-organized documentation ensures that other providers can quickly understand your findings, diagnoses, and recommendations.
Sample Therapy Intake Note
The example below illustrates how a complete therapy intake note might be structured. Names and identifying details are fictional; actual documentation should follow your organization's templates and any payer-specific requirements. Many behavioral health EHRs — including ICANotes — generate this structure automatically once intake fields are entered, so clinicians spend less time formatting and more time on clinical judgment.
Sample Therapy Intake Note
| Client | J.S. | Age | 34 |
| Date of Intake | April 22, 2026 | Clinician | Sample Provider, LCSW |
| Session Length | 75 minutes | Modality | Telehealth (HIPAA-compliant video) |
Chief Complaint
"I've been more anxious than usual for the last three or four months and I can't seem to shake it."
History of Present Illness
Client reports a gradual increase in anxiety beginning in early 2026, attributing onset to a workplace reorganization that increased their workload and uncertainty about job security. Symptoms include persistent worry, muscle tension, difficulty concentrating, and intermittent insomnia (sleep onset latency 45–90 minutes; 5–6 hours total). Denies panic attacks. Reports that worry feels "hard to control" most days. No prior episodes of this severity. Symptoms have begun to affect work performance and increased irritability with partner. Denies depressed mood, anhedonia, manic symptoms, psychotic symptoms, or significant trauma history.
Past Psychiatric History
One prior course of therapy at age 22 (situational, college-related). No prior psychiatric medications. No prior hospitalizations.
Substance Use
Alcohol: 1–2 drinks, 2–3 evenings per week. Caffeine: 2–3 cups of coffee per day. Denies tobacco, cannabis, or other substance use.
Medical History
Generally healthy. Mild seasonal allergies (cetirizine PRN). No chronic medical conditions. No known drug allergies. Last physical exam: November 2025, unremarkable.
Family Psychiatric History
Mother: history of generalized anxiety; treated with therapy and medication. Father: no known psychiatric history. No known family history of suicide, psychosis, or substance use disorders.
Psychosocial History
Lives with long-term partner; describes relationship as supportive but reports recent tension related to client's irritability. Employed full-time as a software engineer; reports satisfaction with career but increasing workplace stress. Maintains close relationships with two siblings and a small social circle. Identifies hiking and reading as primary coping activities, but reports doing both less frequently in recent months.
Mental Status Exam
Alert and oriented x4. Appearance neat, dress appropriate. Cooperative and engaged. Speech regular rate and rhythm. Mood reported as "on edge"; affect anxious but congruent and reactive. Thought process linear and goal-directed. No suicidal or homicidal ideation, intent, or plan. No perceptual disturbances. Insight and judgment intact.
Risk Assessment
Client denies current or past suicidal ideation, self-harm behavior, or thoughts of harming others. No access to firearms. No identified imminent risk factors. Low acute risk; no safety plan required at this time. Will reassess at each session.
Diagnostic Impression
Generalized Anxiety Disorder, moderate (provisional). Rule out Adjustment Disorder with Anxiety. PHQ-9 administered: score 6 (mild, primarily sleep- and concentration-related). GAD-7: score 14 (moderate).
Strengths and Protective Factors
Strong therapeutic alliance evident in first session. Insight into stressors. Stable housing and employment. Supportive partner and family. History of using exercise and reading as coping strategies.
Client Goals
- Reduce daily worry and improve ability to "shut off" thoughts in the evening.
- Improve sleep onset and total sleep time.
- Reduce irritability in relationship with partner.
Plan
- Weekly individual therapy, CBT-based, focused on cognitive restructuring and worry exposure.
- Introduce sleep hygiene strategies and reduce evening caffeine and alcohol.
- Begin tracking worry triggers between sessions.
- Reassess GAD-7 at session 4 and again at session 8.
- Consider psychiatric referral for medication evaluation if no meaningful symptom reduction by session 6, or sooner if symptoms intensify.
- Provide psychoeducation handout on GAD; release of information offered for primary care coordination.
Next Appointment
Scheduled for April 29, 2026, 4:00 PM, telehealth.
Clinician signature: Sample Provider, LCSW • Date signed: April 22, 2026
Next Steps After the Intake
A well-executed therapy intake lays the foundation for effective treatment, but what happens after the first session is just as important. Whether you’ve conducted a mental health intake, counseling intake, or psychiatry intake, your next steps should solidify the therapeutic relationship and keep the client engaged in their care.
1. Develop a Collaborative Treatment Plan
Using the information gathered during the intake, work with the client to outline short-term and long-term goals. Ensure the plan reflects their priorities as well as your clinical recommendations. In psychiatry intakes, this may also include medication management steps and follow-up schedules.
2. Schedule Follow-Up Appointments Promptly
Before the client leaves, confirm the date and time of the next session. Early scheduling reinforces commitment, maintains momentum, and reduces the risk of no-shows.
3. Provide Educational Resources
Offer handouts, reading materials, or reputable online resources that relate to the client’s presenting concerns. This supports psychoeducation, empowers clients between sessions, and can reinforce treatment adherence.
4. Coordinate with Other Providers When Needed
If the client’s care will involve multiple providers—such as a psychiatrist, primary care physician, or case manager—secure the appropriate releases of information and establish communication channels early in the process.
5. Document Next Steps Clearly
Record all agreed-upon actions, treatment goals, and follow-up plans in the client’s record. Clear documentation ensures continuity of care and compliance with professional standards.
Frequently Asked Questions About Therapy Intake
Related Resources
Explore additional guides and templates to help you conduct thorough intake assessments, improve documentation, and streamline your clinical workflow.
The right tools can make every intake smoother, more compliant, and more clinically useful.
With ICANotes, you can complete thorough intake documentation faster using structured templates designed specifically for behavioral health. Our secure patient portal streamlines paperwork collection before the first session, so you can focus on what matters most — building trust and setting the stage for positive outcomes.
Request a free trial of ICANotes to see how our platform can help you improve your intake process and overall client care.
Spend less time formatting intake notes — and more time with clients
ICANotes is built specifically for behavioral health. Structured intake templates prompt for every required clinical element — presenting concern, history, MSE, risk assessment, diagnosis, and plan — so notes are thorough without the manual formatting.
Our secure patient portal lets clients complete intake paperwork before the session; the responses flow directly into the initial assessment for clinician review and editing.
- Structured intake templates for behavioral health
- Prompts for presenting concern, history, MSE, risk, diagnosis, and plan
- Secure portal intake forms that flow into the initial assessment
- Less manual formatting before and after intake sessions
Start your free 30-day trial — no credit card required.
Takes less than 60 seconds to get started
Recent Posts




Dr. October Boyles
DNP, MSN, BSN, RN
Dr. October Boyles is a behavioral health expert and clinical leader with extensive expertise in nursing, compliance, and healthcare operations. With a Doctor of Nursing Practice (DNP) and advanced degrees in nursing, she specializes in evidence-based practices, EHR optimization, and improving outcomes in behavioral health settings. Dr. Boyles is passionate about empowering clinicians with the tools and strategies needed to deliver high-quality, patient-centered care.