Behavioral Health CPT Codes for Mental Health: Complete Guide to Psychotherapy Codes & Billing
Behavioral health CPT codes are essential for accurate mental health billing, helping clinicians document services correctly, prevent claim denials, and maximize reimbursement. This complete guide to CPT codes for mental health covers psychotherapy CPT codes, psychiatry billing codes, testing and assessment codes, and telehealth modifiers — along with practical strategies to improve billing accuracy and ensure compliance.
")
Last Updated: March 27, 2026

")
What You'll Learn
- How to choose the correct CPT code for psychotherapy, psychiatry, testing, and case management services
- The differences between psychotherapy, E/M, HCPCS, and telehealth codes—and when to use each
- How to avoid common billing mistakes that lead to claim denials and audit risk
- When to use key codes like 90834 vs 90837, 90791 vs 90792, and 90839 for crisis care
- How to properly bill E/M services alongside psychotherapy without double-counting time
- Which testing and assessment codes are time-based vs automated—and how to document them correctly
- How telehealth modifiers and place-of-service codes impact reimbursement and compliance
- What affects reimbursement rates—and how to maximize payment for behavioral health services
- How recent CPT code updates impact billing for health behavior assessment and intervention services
Contents
What Are Behavioral Health CPT Codes?
Psychotherapy CPT Codes: The Complete List
Therapy CPT Codes: Add-On Codes and Modifiers
Psychotherapy Crisis Codes
Psychiatry CPT Codes
Mental Health Testing and Assessment Codes
Behavioral Health Billing Codes for Case Management
Telehealth CPT Codes for Mental Health
New and Updated Mental Health CPT Codes
CPT Code Reimbursement Rates
Tips for Maximizing Reimbursement and Avoiding Claim Denials
Use ICANotes for Fast and Accurate Behavioral Health Billing
FAQ: Mental Health CPT Codes
Behavioral health CPT codes are essential to the insurance billing process for every mental health provider. Whether you bill for psychotherapy, psychiatric evaluations, or psychological testing, using the correct CPT codes for mental health determines whether you get reimbursed — and how quickly.
Current Procedural Terminology (CPT) is a uniform coding system developed by the American Medical Association in 1966 to standardize medical record-keeping. Today, mental health CPT codes describe the specific services a clinician provides to a patient — from a 30-minute psychotherapy session to a full psychiatric diagnostic evaluation — and are required on every insurance claim.
This guide covers the complete list of behavioral health CPT codes, including psychotherapy codes, psychiatry billing codes, E/M codes, crisis codes, telehealth modifiers, and testing codes. We also include tips for maximizing reimbursement and avoiding claim denials.
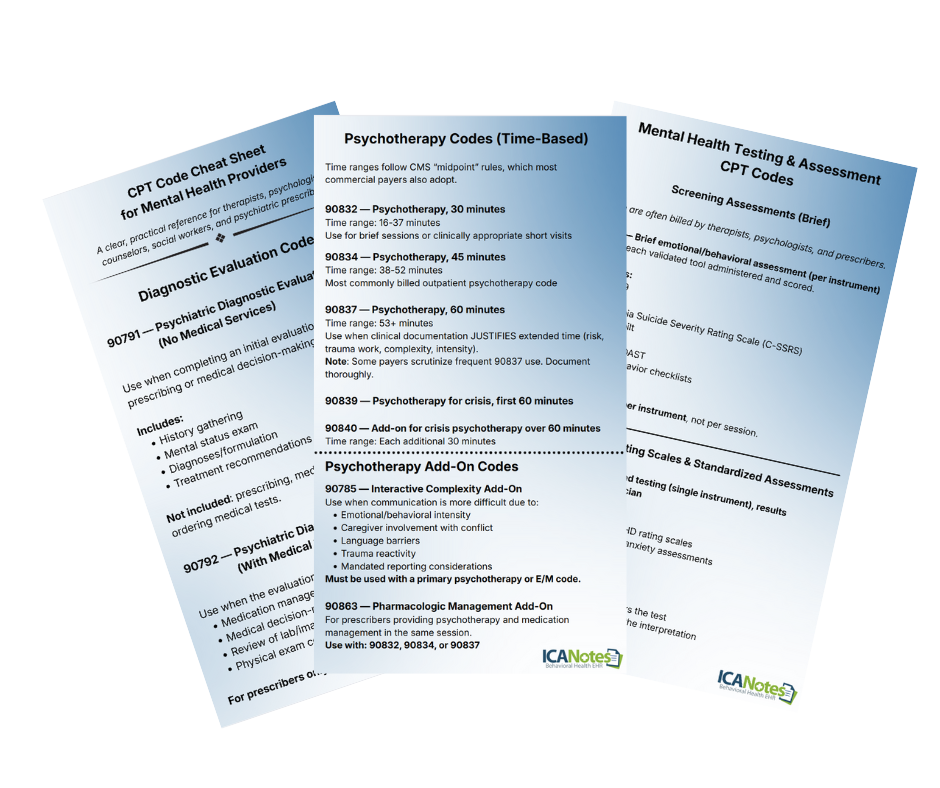
Download the Behavioral Health Coding Cheat Sheet
Get a practical, clinician-friendly reference you can keep nearby when documenting and billing behavioral health services. This cheat sheet is designed to help therapists, psychologists, counselors, social workers, and psychiatric prescribers code more confidently.
Inside, you’ll find commonly used mental health billing codes, telehealth modifiers, testing and assessment codes, E/M guidance, and documentation reminders that can help reduce denials and coding uncertainty.
- Diagnostic evaluation codes for 90791 and 90792
- Psychotherapy and crisis codes with time-based guidance
- E/M and add-on code reminders for prescribers
- Testing, assessment, and telehealth coding tips
What Are Behavioral Health CPT Codes?
CPT codes describe the medical procedures and services a provider performs. For behavioral health, these codes communicate to insurance payers exactly what service was delivered — such as the type and length of a psychotherapy session, a diagnostic interview, or a psychological test.
Along with ICD diagnostic codes, behavioral health CPT codes form the complete picture that insurance companies need to process a reimbursement claim. The ICD code explains why treatment was necessary (the diagnosis), and the CPT code explains what services were provided.
Common mental health ICD codes include:
| ICD Code | Diagnosis |
|---|---|
| F41.9 | Anxiety disorder |
| F31.31 | Bipolar disorder, mild |
| F33 | Major depressive disorder, recurrent |
| F42 | Obsessive-compulsive disorder |
| F43.11 | Post-traumatic stress disorder, acute |
For example, a therapist might pair ICD code F41.9 (anxiety) with CPT code 90834 (45 minutes of individual psychotherapy) to bill for a session with a client experiencing anxiety. Both codes appear on the insurance claim form.

The Three Categories of CPT Codes
CPT codes are organized into three categories:
Category I codes are used most often by mental health providers. These five-digit codes are divided into six sections: Evaluation and Management, Medicine, Surgery, Radiology, Anesthesiology, and Pathology and Laboratory. Psychotherapy CPT codes (90832–90853) fall under the Medicine section's psychiatry subsection. Category I CPT codes are divided into six major sections, each representing a different type of medical service. The numerical ranges for Category I are:
| Section | Code Range |
|---|---|
| Evaluation and Management | 99202–99499 |
| Anesthesia | 00100–01999, 99100–99150 |
| Surgery | 10021–69990 |
| Radiology | 70010–79999 |
| Pathology and Laboratory | 80047–89398 |
| Medicine | 90281–99199, 99500–99607 |
Category II codes are optional supplemental tracking codes. They contain four digits followed by the letter "F" and provide additional performance measurement data. They are not a replacement for Category I or III codes.
Category III codes are temporary codes for new or experimental procedures. They are four digits followed by the letter "T." If a new service isn't yet in Category I, a Category III code may apply.
Psychotherapy CPT Codes: The Complete List
Psychotherapy codes are the most frequently used behavioral health CPT codes for therapists, counselors, and clinical social workers. The American Psychological Association maintains the standard list of psychotherapy CPT codes used by providers.
These psychotherapy CPT codes are time-based, so accurate session duration is critical for proper billing and reimbursement.
| CPT Code | Service Description | Time Range |
|---|---|---|
| 90832 | Individual psychotherapy, 30 minutes | 16–37 minutes |
| 90834 | Individual psychotherapy, 45 minutes | 38–52 minutes |
| 90837 | Individual psychotherapy, 60 minutes | 53+ minutes |
| 90845 | Psychoanalysis | N/A |
| 90846 | Family psychotherapy without the patient present | 26+ minutes |
| 90847 | Family psychotherapy with the patient present | 26+ minutes |
| 90849 | Multiple-family group psychotherapy | N/A |
| 90853 | Group psychotherapy | N/A |

Use 90834
Appropriate for standard psychotherapy sessions where clinical needs can be addressed within a typical timeframe.
Common for routine follow-ups, skill-building, and ongoing treatment.
Use 90837
Use when extended time is clinically necessary due to complexity, severity, or multiple treatment issues.
Often justified for crisis-adjacent care, trauma work, or high-risk patients.
- Selecting the wrong time-based code: Billing 90837 for sessions under 53 minutes is a frequent cause of denials and audits.
- Rounding session time incorrectly: CPT codes must align with documented time ranges—not scheduled session length.
- Using add-on codes without a primary service: Codes like 90785 require a qualifying base service and proper documentation.
- Failing to document medical necessity: Notes must clearly explain why the level of service (e.g., 60-minute session) was clinically appropriate.
- Not distinguishing psychotherapy from E/M services: When both are provided, documentation must separate therapeutic time from medical decision-making.
- Overusing higher-paying codes: Consistently billing 90837 without justification can trigger payer scrutiny or audits.

How to Choose the Right Psychotherapy Code
When selecting a psychotherapy CPT code, choose the code closest to the actual time spent delivering psychotherapy during the session. Though codes describe specific durations like 30, 45, or 60 minutes, therapists have flexibility because sessions often run slightly over or under. The APA defines these time ranges:
- 90832: Sessions between 16 and 37 minutes
- 90834: Sessions between 38 and 52 minutes
- 90837: Sessions lasting 53 minutes or longer
- 90846 or 90847: Family psychotherapy sessions of 26 minutes or more
The time-based ranges are important — selecting the wrong code is a common cause of claim denials and potential audits.
Therapy CPT Codes: Add-On Codes and Modifiers
Beyond the core psychotherapy codes, providers often need add-on codes to describe additional services delivered during the same encounter. Add-on codes for therapy can only be used in combination with a primary psychotherapy or diagnostic evaluation code, and both must be listed separately on the billing form.
| CPT Code | Description |
|---|---|
| 90785 | Interactive complexity |
| 90863 | Psychopharmacology with psychotherapy |
| 90833 | 30 minutes of psychotherapy with E/M service |
| 90836 | 45 minutes of psychotherapy with E/M service |
| 90838 | 60 minutes of psychotherapy with E/M service |
- Choosing the wrong time-based code: Billing 90837 for a session under 53 minutes is one of the most common causes of claim denials.
- Using add-on codes incorrectly: Codes like 90833, 90836, and 90838 must be billed with an E/M service—not psychotherapy alone.
- Missing or incorrect modifiers: Failing to include modifier 95 for telehealth or using incorrect modifiers can result in reduced or denied reimbursement.
- Insufficient documentation: Your clinical notes must clearly support the level of service billed, including time, interventions, and medical necessity.
- Double-counting time: Time spent on E/M services cannot be counted toward psychotherapy time when billing both.
- Billing services that lack medical necessity: Even correctly coded services may be denied if documentation doesn’t justify the need for treatment.
When to use code 90785 (Interactive Complexity): Use this add-on code when complicating factors affect service delivery — such as the presence of an angry family member, a third party like a probation officer, the use of play equipment or interpreters, or when the patient's emotional state significantly complicates communication.
When to use code 90863: Psychologists may use code 90863 when reviewing or prescribing medication on the same day as delivering psychotherapy services. Note that psychiatrists do not use this code — they use E/M codes instead (see the Psychiatry section below).
CPT Code Modifiers for Mental Health
CPT codes can also have modifiers — two-digit numbers or letters appended to a code — that describe specific details about how a service was delivered. Modifiers specify things like whether multiple services were provided, the reason for the service, and where services occurred. Proper modifier use is critical: improper modifiers are a leading cause of claim denials, and correct modifiers can mean the difference between maximum reimbursement and reduced payment.
Psychotherapy Crisis Codes
CPT codes for psychotherapy crises allow behavioral health professionals to bill for emergency sessions with patients in significant distress who require immediate attention or are in a life-threatening situation.
| CPT Code | Description |
|---|---|
| 90839 | Psychotherapy for crisis, first 60 minutes |
| 90840 | Each additional 30 minutes of psychotherapy for crisis (add-on) |
| 99050 | Services provided when the office is usually closed (add-on) |
| 99051 | Services during regularly scheduled hours on evenings, weekends, or holidays (add-on) |
If a crisis session falls below 60 minutes, bill using a standard psychotherapy code such as 90834 instead of 90839.
- Routine therapy sessions: Even if a client is distressed, standard psychotherapy codes (90832, 90834, 90837) apply unless criteria for crisis are met.
- Sessions under 60 minutes: If the encounter is less than 60 minutes, bill a standard psychotherapy code instead.
- No immediate safety risk: 90839 is reserved for urgent situations involving significant risk (e.g., suicidality, acute crisis).
- Lack of crisis-level intervention: Documentation must show active crisis management—not just discussion of stressors.
- Planned or scheduled sessions: Regularly scheduled appointments typically do not qualify as crisis services.
Psychiatry CPT Codes
Psychiatrists use a combination of CPT codes to bill for diagnostic evaluations, psychotherapy, and specialized psychiatric services. The following psychiatry CPT codes cover services unique to psychiatric practice:
| CPT Code | Description |
|---|---|
| 90791 | Psychiatric diagnostic evaluation without medical services |
| 90792 | Psychiatric diagnostic evaluation with medical services |
| 90865 | Narcosynthesis |
| 90867 | Therapeutic repetitive transcranial magnetic stimulation (TMS) |
| 90870 | Electroconvulsive therapy (ECT) |
| 90875 | Individual psychophysiological therapy with biofeedback, 30 minutes |
| 90876 | Individual psychophysiological therapy with biofeedback, 45 minutes |
| 90880 | Hypnotherapy |
| 90899 | Unlisted psychiatric procedure or service |
90791 – Without Medical Services
Used for a psychiatric diagnostic evaluation without medical components. Typically billed by therapists, psychologists, or non-prescribing clinicians conducting an intake assessment.
90792 – With Medical Services
Used for a psychiatric diagnostic evaluation that includes medical services, such as medication review, prescribing, or physical assessment. Typically used by psychiatrists, NPs, or physicians.
Psychiatry Evaluation and Management (E/M) Codes
Psychiatrists and other physicians may use E/M codes to bill for evaluation and management services, either alone or combined with psychotherapy. When a psychiatrist provides psychotherapy, the psychotherapy code is treated as an add-on to the primary E/M service.
| Code Range | Description |
|---|---|
| 99202–99205 | Outpatient E/M for new patients |
| 99211–99215 | Outpatient E/M for established patients |
| 99241–99245 | Outpatient consultations (new or established) |
| 99221–99223 | Initial hospital E/M (new or established) |
| 99231–99233 | Subsequent hospital E/M |
| 99251–99255 | Inpatient consultations |
Accurately separating E/M and psychotherapy services in real time can be challenging — especially when documentation requirements differ.
How to Use E/M Codes Correctly in Psychiatry
For new patients, you may bill two types of codes: E/M codes and psychiatric diagnostic evaluation codes. Depending on the situation and time involved, it may be appropriate to bill for both.
- E/M codes: Use when evaluating a new medical issue. With the AMA's current coding guidelines, you can select an E/M code based on the complexity of medical decision-making or the total time spent on the patient's care that day. However, if you provide E/M services with a psychotherapy add-on code, you must choose a code based on medical decision-making — not total time.
- Psychiatric diagnostic evaluation: Use codes 90791 or 90792 for diagnostic assessments. You may need to use these codes more than once if the initial evaluation takes multiple sessions to complete.
For established patients, you may bill an E/M service with every psychotherapy visit, but you are not required to. Only bill E/M if you addressed and documented a separate medical issue during the visit. For example, if you discuss medication side effects during an encounter, you might bill for E/M in addition to psychotherapy. But if a patient is stable on the same medication and attends a routine psychotherapy session, you can only bill for the psychotherapy — there are no separate medical or medication concerns to justify E/M.
Your documentation must prove active management or discussion of a medical or medication problem distinct from the psychotherapy service.
The Three Components of E/M Documentation
Insurance companies require documentation to confirm the medical necessity of services and the accuracy of reported codes. Your records must include:
- History: History of present illness, review of body systems, and family and social history.
- Examination: The type and extent of examination based on your clinical judgment and the presenting problem. Levels range from problem-focused through comprehensive.
- Medical decision-making: The number and complexity of problems addressed, the complexity of data reviewed, and the risk of complications.
When selecting an E/M code with a psychotherapy add-on, base your E/M code on medical decision-making. Then choose the timed psychotherapy add-on (90833, 90836, or 90838) based on the duration of psychotherapy delivered. Keep E/M and psychotherapy time separate — time spent on E/M cannot count toward psychotherapy time.
Mental Health Testing and Assessment Codes
CPT codes for mental health testing and assessments are used to bill for structured evaluations, screenings, and psychological or neuropsychological testing services.
| CPT Code | Description |
|---|---|
| 96105 | Aphasia assessment |
| 96110 | Developmental screening |
| 96112 | Developmental test administration with interpretation |
| 96113 | Each additional 30 minutes of developmental test administration |
| 96116 | Neurobehavioral status exam, 60 minutes |
| 96121 | Each additional hour of neurobehavioral status exam |
| 96125 | Standardized cognitive performance testing, 60 minutes |
| 96127 | Brief emotional or behavioral assessment |
| 96130 | Psychological testing evaluation, 60 minutes (physician/QHP) |
| 96131 | Each additional hour of psychological testing evaluation |
| 96132 | Neuropsychological testing services, 60 minutes |
| 96133 | Each additional hour of neuropsychological testing services |
| 96136 | Psych/neuropsych test administration and scoring, 30 minutes (physician/QHP) |
| 96137 | Each additional 30 minutes of test administration and scoring (physician/QHP) |
| 96138 | Psych/neuropsych test administration and scoring, 30 minutes (technician) |
| 96139 | Each additional 30 minutes of test administration and scoring (technician) |
| 96146 | Psych/neuropsych test via electronic platform with automated results |
| 96156 | Health behavior assessment or reassessment |
| 96160 | Patient-focused health risk assessment |
| 96161 | Caregiver-focused health risk assessment |
- Physicians / Psychiatrists / QHPs: Can bill for testing evaluation and interpretation codes such as 96130–96133.
- Psychologists: Can bill both administration and interpretation codes.
- Technicians: Can bill administration/scoring only (96138–96139).
- Therapists / Counselors: Typically limited to brief assessments like 96127.
- Automated platforms: Use 96146 for fully automated testing.
- Insufficient documentation: Notes do not clearly support the need for testing, the services performed, or the time spent.
- Wrong code selection: The billed code does not match whether the service was automated, technician-administered, or interpreted by a qualified provider.
- Missing medical necessity: The claim does not adequately connect the testing service to the presenting problem, diagnosis, or treatment need.
- Improper use of add-on time codes: Additional time-based codes are billed without enough documented time to support them.
- Credentialing or scope issues: The provider billing the service is not recognized by the payer as eligible to bill that particular testing code.
1. Testing
Select and administer the appropriate screening, psychological, or neuropsychological test based on the clinical concern and scope of service.
2. Scoring
Score the instrument accurately, whether manually, electronically, or through a technician-supported workflow, and record the method used.
3. Interpretation
Document the clinical meaning of the results, including how findings relate to diagnosis, symptoms, functioning, or treatment planning.
4. Billing
Choose the code that matches who performed the service, whether time was involved, and whether the work included administration, evaluation, or automated reporting.
Behavioral Health Billing Codes for Case Management
Clinical social workers and licensed counselors use many of the same behavioral health billing codes as other providers when billing for psychotherapy and case management services. The most commonly used behavioral health billing codes for case management, according to CMS, are:
| CPT Code | Description |
|---|---|
| 90832 | 30 minutes of psychotherapy |
| 90834 | 45 minutes of psychotherapy |
| 90837 | 60 minutes of psychotherapy |
| 90785 | Interactive complexity add-on |
| 90839 | 60 minutes of psychotherapy for crisis |
| 90840 | Each additional 30 minutes of crisis psychotherapy |
| 90791 | Psychiatric diagnostic evaluation |
| 90845 | Psychoanalysis |
| 90846 | Family psychotherapy without the patient present, 50 minutes |
| 90847 | Family psychotherapy with the patient present, 50 minutes |
| 90853 | Group psychotherapy |
- Using psychotherapy codes for non-therapy services: Case management tasks like care coordination or referrals are not always billable under standard psychotherapy CPT codes.
- Billing crisis codes without meeting criteria: Codes like 90839 require clear documentation of acute distress and immediate intervention—not routine high-need sessions.
- Missing interactive complexity documentation: Code 90785 must be supported by specific complicating factors, such as involvement of third parties or communication barriers.
- Incorrect session duration: Time-based psychotherapy codes must align with documented session length to avoid denials.
- Overlapping services: Billing multiple services in a single encounter without clearly distinguishing them in documentation can trigger claim rejections.
- Lack of medical necessity: Even appropriate codes may be denied if the documentation does not justify the clinical need for services.
Telehealth CPT Codes for Mental Health
Since many behavioral health professionals now offer virtual sessions, understanding telehealth coding is essential. According to the Centers for Medicare and Medicaid Services, telehealth visits are treated the same as in-person visits and are reimbursed at the same rates. You use the same CPT code for a virtual session as you would for a face-to-face meeting — for example, 90834 for a 45-minute psychotherapy session conducted via video.
The key difference is in the modifiers and place-of-service codes:
| Modifier / Code | Description |
|---|---|
| Modifier 95 (or GT) | Real-time audio/video interaction via telecommunications |
| POS 02 | Place of service: telehealth (replaces POS 11 for office) |
Some telehealth services use HCPCS codes (Healthcare Common Procedural Coding System) rather than CPT codes. HCPCS codes are not part of the CPT set and consist of a letter followed by four numbers:
- Forgetting modifier 95 (or GT): Without the correct modifier, telehealth claims may be denied or reimbursed incorrectly.
- Using the wrong place of service (POS): Failing to use POS 02 (or payer-specific requirements) is a frequent cause of claim rejection.
- Billing audio-only sessions incorrectly: Some payers require different codes or do not reimburse audio-only services the same as video visits.
- Not verifying payer-specific rules: Telehealth coverage and requirements vary widely by payer and state.
- Missing documentation of modality: Notes should clearly indicate that the session was conducted via real-time audio/video.
- Assuming parity without confirmation: While many payers reimburse telehealth at the same rate as in-person care, this is not universal.
| Code | Description |
|---|---|
| G2012 | Virtual check-in (brief, patient-initiated) |
| G2010 | Remote evaluation of recorded video/image from established patient |
| 99421 | Online digital E/M via patient portal, 5–10 min over 7 days |
| 99422 | Online digital E/M via patient portal, 11–20 min over 7 days |
| 99423 | Online digital E/M via patient portal, 21+ min over 7 days |
Non-physician health professionals may use codes G2061, G2062, or G2063 to provide an online assessment and management service for an established patient.
New and Updated Mental Health CPT Codes
The AMA updates CPT codes annually, and mental health providers should stay current with the latest changes to ensure proper reimbursement. The most recent updates include new HCPCS and CPT codes along with updated language to improve provider understanding.
Health behavior assessment and intervention codes require a physical health diagnosis (ICD code) and are distinct from mental health service codes. Here are the key recent code revisions:
| Old Code(s) | New Code(s) | Change |
|---|---|---|
| 96150, 96151 | 96156 | Health and behavior assessment/reassessment — now event-based, not time-based |
| 96152 | 96158 + 96159 | Individual health behavior intervention: 96158 for first 30 min, 96159 for each additional 15 min |
| 96153 | 96164 + 96165 | Group health behavior intervention: 96164 for first 30 min, 96165 for each additional 15 min |
| 96154 | 96167 + 96168 | Family intervention with patient: 96167 for first 30 min, 96168 for each additional 15 min |
| 96155 | 96170 + 96171 | Family intervention without patient: 96170 for first 30 min, 96171 for each additional 15 min |
Health behavior assessment and intervention codes were restructured to better reflect how services are actually delivered in clinical practice. The shift from time-based to event-based coding (e.g., 96156) simplifies billing for certain assessments while introducing more granular options for intervention services.
The newer code sets (96158–96171) separate initial service time from additional increments, allowing for more precise billing and improved reimbursement alignment. However, they also require more detailed documentation to support both time and clinical purpose.
For clinicians, this means greater flexibility—but also a higher risk of errors if documentation does not clearly support the selected codes. Understanding these changes is essential for maintaining compliance and maximizing reimbursement.
CPT Code Reimbursement Rates
Reimbursement rates for behavioral health CPT codes vary based on the insurance payer, the provider's geographic location, and the practitioner's credential level. In general, psychiatrists receive higher reimbursement rates than social workers for the same code, and longer sessions reimburse at higher rates.
The following example reimbursement rates reflect more recent Mississippi Medicaid fee schedule data for selected behavioral health CPT and HCPCS codes.
| CPT/HCPCS | Description | Rate Type | Fee | Effective Date |
|---|---|---|---|---|
| 90791 | Psychiatric diagnostic evaluation | DEF | $146.31 | 07/01/2024 |
| 90792 | Psychiatric diagnostic eval with medical services | DEF | $163.85 | 07/01/2024 |
| 90832 | Psychotherapy, 30 minutes | DEF | $66.65 | 07/01/2024 |
| 90834 | Psychotherapy, 45 minutes | DEF | $87.94 | 07/01/2024 |
| 90837 | Psychotherapy, 60 minutes | DEF | $129.65 | 07/01/2024 |
| 90847 | Family psychotherapy with patient | DEF | $88.34 | 07/01/2024 |
| 96127 | Brief emotional/behavioral assessment | DEF | $3.49 | 07/01/2024 |
| H0036 | Community psychiatric face-to-face, 15 min | DEF | $63.50 | 11/01/2023 |
| H2011 | Crisis intervention service, 15 min | DEF | $34.74 | 07/01/2024 |
| H2017 | Psychosocial rehabilitation service, 15 min | DEF | $4.48 | 07/01/2024 |
Reimbursement rates for behavioral health CPT codes can vary significantly depending on several factors. Each insurance payer sets its own fee schedule, and government programs like Medicaid and Medicare adjust rates based on geographic location and regional cost of care.
Provider credentials also play a role—psychiatrists and physicians are typically reimbursed at higher rates than licensed therapists for the same CPT codes. Additionally, payer contracts, network participation, and negotiated rates can all impact final reimbursement amounts.
Because of this variability, clinicians should treat published rates as general benchmarks and always verify reimbursement details with each payer to ensure accurate billing and revenue expectations.
The CMS accepts the American Medical Association's CPT code recommendations and makes final decisions about code values. With the current E/M coding rules, clinicians can bill for the total time they spend on an encounter in one day — including non-face-to-face time — and receive credit for tasks like interpreting exams performed by other physicians. Clinicians can also choose an E/M code based on total time or medical decision-making, selecting whichever option results in appropriate reimbursement.
Tips for Maximizing Reimbursement and Avoiding Claim Denials
Medical necessity determines the level of service you should bill. Never document a higher service level than what was actually necessary. Here are the key practices to follow:
1. Ensure Correct Coding
Coding errors lead to payment delays, rejected claims, and — if frequent — potential audits or fraud charges. Always refer to the AMA's most recent CPT manual and double-check your work. Pay special attention to modifiers, which are a leading cause of denials and can mean the difference between full reimbursement and reduced payment.
2. Claim Only What's Medically Necesarry
Medicare and other payers will deny claims for services that are not medically necessary. Choose the appropriate ICD code and link it to the associated CPT codes to demonstrate clearly why each service was provided.
3. File Claims on Time
Medicare requires claims within 12 months of the date of service, but other payers may set deadlines as short as 90 or 180 days. Missing submission deadlines is one of the most common reasons for claim denials. Establish a workflow to complete paperwork well before deadlines, and consider EHR software to help track due dates.
4. Prioritize Quality Documentation
Incomplete or illegible documentation will trigger denials. Verify that clinical notes, patient information (name, date of birth, policy number, group number, relationship to insured), and all required fields are accurate and complete before submission. Minor data-entry errors — like a misspelled name or incorrect Social Security number — are surprisingly common and easily preventable.
5. Train Staff and Review Denials
Create a standard workflow for managing claims. Track the reasons for past denials, educate staff on common errors, and schedule regular training to stay current on code changes. The most frequent causes of denials include duplicate submissions, ineligible services, and settled claims.
6. Verify Insurance and Eligibility
Before every session, confirm that the client's insurance covers your services. Patient ineligibility is a top reason for denials. Complete eligibility verification before the first appointment, collect copayments during the initial visit, and maintain copies of the patient's insurance card and identification.
7. Automate Where Possible
EHR software can streamline documentation, automatically suggest the correct CPT code for the services you document, and ensure your notes meet the standards insurance companies require. Automation reduces manual errors and helps submit clean claims the first time.
Related Behavioral Health Billing Resources
Explore additional guidance on mental health billing.
Use ICANotes for Fast and Accurate Behavioral Health Billing
Using proper CPT codes for mental health requires knowledge and constant attention to code updates. Most behavioral health clinicians want to spend their time providing patient care — not worrying about coding and claims.
ICANotes keeps track of documentation elements in your clinical notes and automatically calculates the highest-level E/M code supported by each note. With pre-templated buttons and an intuitive point-and-click interface, ICANotes makes it easy to establish all the required details for accurate billing while staying compliant with HIPAA and current CPT guidelines.
With ICANotes, you can expect:
- Automatic coding at the highest reimbursement level supported by your documentation
- Fewer errors, resubmissions, and claim denials
- Behavioral health notes completed in as little as 3 minutes
- Free training and 24/7 support
- Full HIPAA compliance
Sign up for a free 30-day trial of ICANotes today.
")
Start Your 30-Day Free Trial
Experience the most intuitive, clinically robust EHR designed for behavioral health professionals, built to streamline documentation, improve compliance, and enhance patient care.
- Complete Notes in Minutes - Purpose-built for behavioral health charting
- Always Audit-Ready – Structured documentation that meets payer requirements
- Keep Your Schedule Full – Automated reminders reduce costly no-shows
- Engage Clients Seamlessly – Secure portal for forms, messages, and payments
- HIPAA-Compliant Telehealth built into your workflow
Frequently Asked Questions About Mental Health CPT Codes
Related Posts



Dr. October Boyles
DNP, MSN, BSN, RN
About the Author
Dr. October Boyles is a behavioral health expert and clinical leader with extensive expertise in nursing, compliance, and healthcare operations. With a Doctor of Nursing Practice (DNP) and advanced degrees in nursing, she specializes in evidence-based practices, EHR optimization, and improving outcomes in behavioral health settings. Dr. Boyles is passionate about empowering clinicians with the tools and strategies needed to deliver high-quality, patient-centered care.