
Automatic E&M Coding for Behavioral Health — Built Into Every Note
ICANotes calculates your E&M CPT code as you chart — matching your Medical Decision Making complexity to the correct level so you bill accurately, get paid faster, and stay audit-ready.
Trusted by psychiatrists, APRNs, PMHNPs, and behavioral health prescribers across the U.S.
Most Behavioral Health Prescribers Are Leaving Money on the Table
Coding behavioral health E&M visits correctly is harder than it should be. When documentation does not clearly support Medical Decision Making complexity, even experienced prescribers can undercode, underbill, and understate the real intensity of care delivered.
CMS data shows that over 40% of outpatient behavioral health visits are coded below their actual MDM level. A 2023 MGMA benchmark found that up to 60% of psychotherapy with E&M codes are billed incorrectly due to time-versus-MDM confusion.
That means many prescribers are routinely undercoding — not out of negligence, but because translating complex clinical work into E&M levels is genuinely difficult without the right tools.
The cost is real. A practice seeing just 100 established patients per month could be leaving more than $30,000 in legitimate annual revenue uncollected each year — revenue that accurately reflects the care already delivered.
Undercoding also misrepresents patient acuity in your records, makes practice-level reporting less accurate, and fails to tell the true clinical story of the patients you are treating.
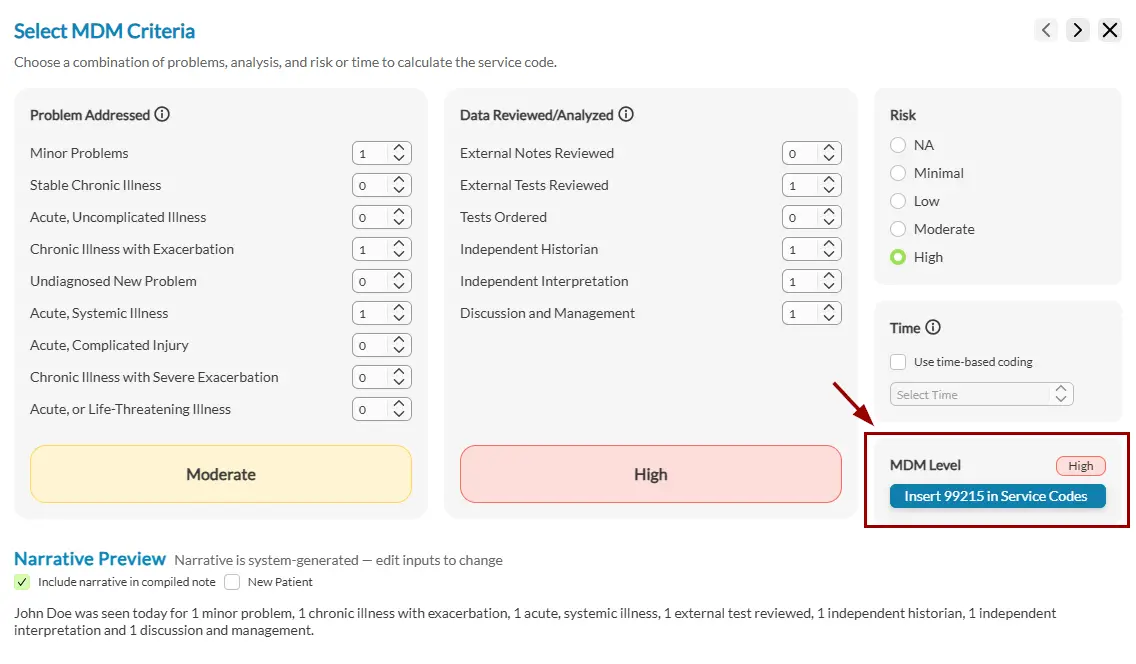
How ICANotes Automatic E&M Coding Works
ICANotes is the only behavioral health EHR with a built-in MDM coding matrix that calculates your E&M level in real time as you document — eliminating guesswork and helping protect you in an audit.
Audit-Ready Documentation, Built Into the Workflow
The OIG has found that 88% of denied behavioral health claims trace back to documentation errors — not fraud. That is a solvable problem, and it is exactly what ICANotes is designed to address.
Automatic E&M coding does more than help clinicians choose the right code. It helps ensure that the reasoning behind the code is clearly documented inside the note, where auditors and payers expect to see it.
Built for Behavioral Health Prescribers
Automatic E&M coding in ICANotes is designed for clinicians who prescribe and manage medications as part of mental health treatment.
Psychiatrists
Manage complex patient panels, medication changes, safety concerns, and high-acuity visits with documentation that supports the full complexity of psychiatric decision-making.
Psychiatric Nurse Practitioners
Support solo and group-practice PMHNP workflows with built-in coding guidance that helps align documentation, reimbursement, and defensible billing decisions.
Physician Assistants
Document medication management visits more confidently with coding support that reflects real-world behavioral health complexity and site-of-service variation.
Integrated Care Practices
Standardize E&M coding across prescribing clinicians while improving documentation consistency, audit readiness, and reimbursement accuracy across the organization.
Note: E&M codes such as 99212–99215 apply to prescribing clinicians. Non-prescribing clinicians such as LCSWs, LPCs, and LMFTs typically bill psychotherapy codes like 90832, 90834, and 90837. ICANotes supports accurate coding for both.
Why Behavioral Health Prescribers Choose ICANotes
ICANotes has been built specifically for behavioral health for nearly a decade — not adapted from a general-purpose EHR. That focus means every feature, including automatic coding, reflects the real complexity of psychiatric documentation.
Common Questions About Automatic E&M Coding
Get quick answers to common questions about MDM coding, time-based coding, claim denials, and behavioral health documentation requirements.
Stop Undercoding. Start Getting Paid for the Work You Do.
ICANotes takes the guesswork out of E&M coding so you can document confidently, bill accurately, and keep your focus on patient care.
No commitment required. See how ICANotes’ automatic coding matrix works in a live, personalized walkthrough.